
Michael Snyderman, MD
In the 1970’s three independent laboratories reported the presence of a MLRV in sarcoma, leukemia and various lymphomas [1-6]. The MLRV was found only in neoplastic and not in normal cells and was similar to the Rauscher virus. The most recent nomenclature calls this type of virus an HGRV. Surprisingly, the 1970’s body of work was largely ignored for the next thirty years until 2006 when Urisman et al [7] reported a HGRV/MLRV which they named XMRV in some prostate cancer. In 2009, Lombardi et al [8] at the Whittemore Peterson Institute (WPI) found evidence of infection with HGRV/MLRVs similar to XMRV in most patients with the Chronic Fatigue Syndrome (CFS). At present, the Lombardi et al viral findings have been criticized because many laboratories have not been able to reproduce their results. Some retrovirologists have said unequivocally that HGRV/MLRVs do not cause CFS.
The diagnosis of CFS is objectified by using the Canadian Criteria for diagnosis of CFS and by demonstrating a typical elevation of cytokines and chemokines [9]. CFS patients are suspected to have an increased incidence of lymphoid malignancy and brain tumors compared to the normal population [10]. The implication of this is that HGRV/MLRVs may be etiological for both CFS and malignancy. Daniel Peterson’s CFS practice consisted of 300 patients from the 1984 Nevada CFS epidemic. Thirteen patients from this cohort developed various B-cell lymphoproliferative disorders and all that were tested were positive for a T-cell clonal expansion. They were also found to have evidence of infection with HGRV/MLRV at the WPI but this latter data is now in limbo. It was hypothesized that a HGRV/MLRV infection was responsible for the T-cell clonal expansion and that this clonal T-cell expansion might have promoted the development of CFS and malignancy.
Treatment of MLRV associated malignancy has not previously been reported. The retrovirus HTLV-1 associated T-cell lymphoma/leukemia does respond to AZT and IFNa [11, 12]. In addition, multiple human tumor cell lines including breast and ovarian cancers show growth inhibition and apoptosis when exposed to AZT [13, 14]. Several groups reported inhibition of XMRV by FDA approved antiretrovirals including AZT, raltegravir and tenofovir in cell culture [15, 16]. The response of a patient with CFS and a MLRV associated malignancy to anti-retroviral drug therapy would support a role of MLRV in both. We had the opportunity to study such a patient with both CFS and CLL who was positive for evidence of infection with MLRV and was also positive for a T-cell clonal expansion. He had cytokine and chemokine elevations consistent with the diagnosis of CFS. This patient was a Medical Oncologist who was well acquainted with the therapeutic options and guidelines for both disorders and decided to undergo anti-
retroviral therapy.
Results
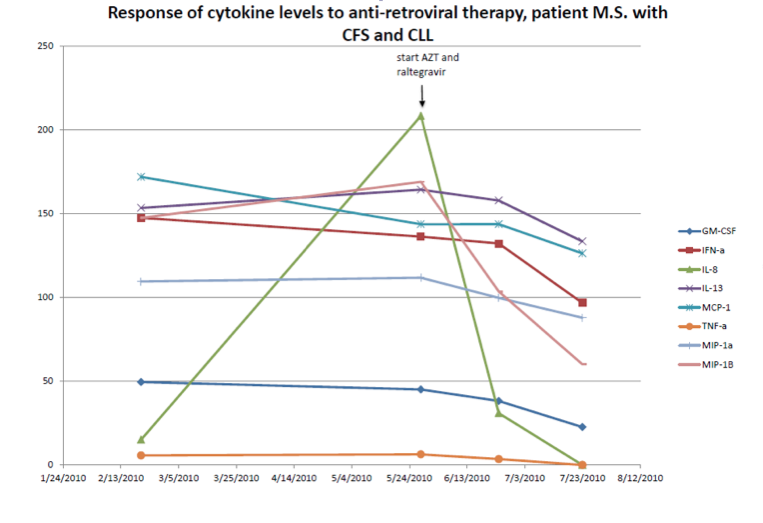
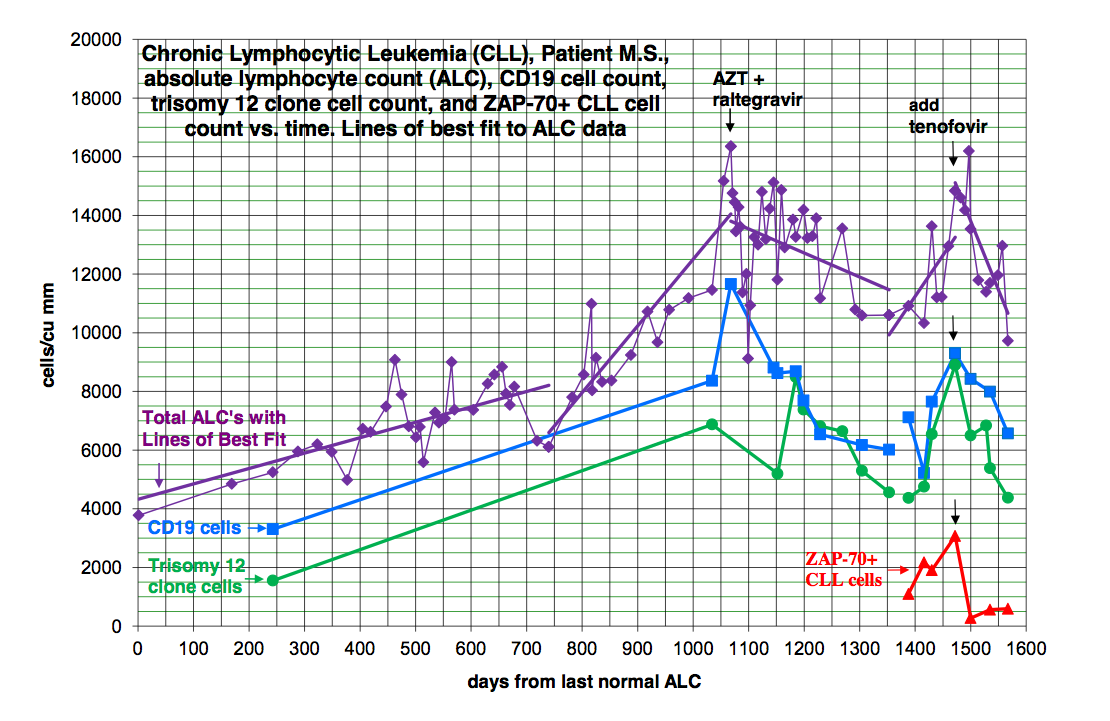
A patient with B-cell CLL tested positive for antibodies to MLRV proteins. Integration studies are pending. Although not previously diagnosed as having CFS, his symptoms fulfilled the Canadian Criteria for diagnosis of CFS. His elevated cytokine and chemokine levels were consistent with the diagnosis of CFS. He was also positive for a clonal T-cell expansion by both quantitative and qualitative assays for the presence of a clonal TCRg gene rearrangement. He had average prognostic factors with the only potential adverse factor being a trisomy 12 clone. His testing for EBV, CMV, HHV6A and HHV6B was negative. He started treatment with AZT and raltegravir 571 days after diagnosis of CLL. By day 56 of treatment, his cytokine levels had improved (Figure 1). This coincided with improvement in symptoms of CFS which included fatigue, difficulty in concentration and neuropathic pain. His response continued for 9.4 months with no associated toxicity and he was able to work full time. His previously increasing absolute lymphocyte count (ALC), CD 19 cells and trisomy 12 cells trended downward during this period of time. At the start of treatment with AZT and raltegravir, his ALC was 16,348/cu mm and CD 19 cells 11,658/cu mm up from 3,303 at diagnosis. His trisomy 12 cells peaked at 8,490/cu mm day 117 of treatment up from 1,550 at diagnosis. After 285 days of treatment his ALC was down to 10,600/cu mm, CD 19 cells down to 6,015 and trisomy 12 down to 4,558. Subsequently, his counts relapsed despite continuation of AZT and raltegravir. Symptoms of CFS also worsened. Tenofovir was added and all parameters trended down again and symptoms of CFS improved (Figure 2). The ALC peaked at 16,194 at week 3 of treatment and by week 20 was down to 12,324. The baseline CD-19 count was 9,298, trisomy 12 cell count was 8,902 and the ZAP70 count was 3,068. By week 13 the CD-19 count was down to 6,570, the trisomy 12 count was down to 4,374 and the ZAP70 count was down to 591. Week 20 values of these last three parameters are pending. Quantitative data for clonal T-cells became available at the time of relapse and showed a rise in clonal T-cells that appeared to be more rapid than the increase in the CD-19 cells and after the addition of tenofovir both the clonal T-cells and the CD-19 cells trended down but the clonal T-cells appeared to decrease more rapidly (Figure 3).
Discussion
The development of B-cell lymphoid malignancies in 13 of 300 CFS patients suggests that CFS patients are at a several hundred fold increased risk for malignancy compared to generally quoted incidences for the general population. Of these 13 patients, all were positive for a clonal T-cell expansion. They were also positive for evidence of infection with HGRV/MLRVs but this data is now in question.
The greatly increased risk for B-cell malignancy in a potentially HGRV/MLRV infected population may be due to infection of the B-cell line by the HGRV/MLRVs. Retroviruses have been thought to cause cancer by insertional mutagenesis. This mechanism requires that the retrovirus proviral DNA be integrated into host cell DNA next to a proto-oncogene thereby inducing activation of the proto-oncogene. A more important mechanism with MLRVs may be the ability of viral proteins to change host cell gene expression. Twenty-four to forty-eight hours after a permissive cell line is infected with XMRV, multiple cellular genes are expressed: “10 genes are implicated in cell morphology, 11 genes in cellular development, 12 genes in cell-to-cell signaling and interaction, 11 genes in cellular movement and 13 genes in cellular growth and proliferation” [17]. Spadafaro has shown that reverse transcriptase can cause gene activation and lead to the malignant phenotype [18]. In some retrovirus related cancers, Env [19] and Gag [20] may also be important in malignant transformation.
The finding that XMRV did not cause malignant transformation de novo in tissue culture [21] would be irrelevant to the clinical reality of human cancer. It is accepted that multiple events are necessary to convert a cell line into a pre-neoplasm or a clinically important neoplasm. Human cancers have mutated genes and changes in gene expression that could make them permissive to infection by retroviruses. The retroviruses could induce further changes in gene expression that would make the infected cell line behave in a more malignant fashion. The corollary to this is that treatment that would block viral protein influence in a neoplastic cell line could make the neoplastic cell behave in a less malignant way.
A complementary hypothesis is that infection by HGRV/MLRVs results in a T-cell clonal expansion. The clonal T-cells produce elevated cytokine and chemokine levels which may be partially responsible for the CFS. Furthermore these cytokines and chemokines may have a paracrine activity that would stimulate a simultaneous neoplasm to behave in a more aggressive fashion [22].
One objection to considering HGRV/MLRVs to be pathogenic viruses is that there was previously no explanation as to how MLRVs could have entered the human population. However, early vaccines were prepared by passaging human virus through mice for the purposes of viral isolation and for attenuation. This would have allowed for contamination of vaccines with murine leukemia viruses [23]. The original Yellow Fever Vaccine was made in the early 1930’s by culturing the virus in mouse cerebral tissue [24]. Some patients received both the Yellow Fever virus and infected mouse cerebral tissue. The YF17D strain was used to immunize over 400 million people world-wide over the next 65 years [25]. The U.S. Armed Forces started to vaccinate service men for Yellow Fever during WWII and continued thereafter as per the branch of service and deployment status [26]. The polio vaccination trials in the United States started in 1952. The polio virus strains were initially serially transferred by Koprowski through many passages in mice, cotton rats and primates to achieve attenuation [27]. Olitsky with whom Sabin had a long-term collaboration adapted the type 2 (Lansing) polio strain to mice [28] and the Sabin vaccine contained this strain. Indeed, the patient studied here, received the live oral polio vaccine in the early 1960s, ten years later developed symptoms of CFS and forty years later developed CLL. He also received the Yellow Fever vaccine in the early 1970’s on entering the Armed Services.
In summary, a new patient with both CFS and B-cell CLL was identified. Infection with a HGRV/MLRV was suggested by the presence of antibodies to MLRV proteins. He also was positive for a T-cell clonal expansion and had elevated cytokine and chemokine levels typical of patients with CFS. With anti-retroviral therapy he showed improvement in his cytokine and chemokine levels, CFS symptoms and hematological parameters. Presumably his improvement was related to the anti-retroviral effects of treatment. The progressive improvement of his ALC, CD19 cells and trisomy 12 clone lasted 9.4 months. Despite continuation of AZT and raltegravir his leukemia relapsed. Interestingly, during relapse both the total B-cell count and the clonal T-cells increased with the rate of increase of the T-cells appearing more rapid. A second response was induced by the addition of the second reverse transcriptase inhibitor, tenofovir. Both the total lymphocyte count and the clonal T-cells fell with the rate of decrease of the clonal t-cells appearing more rapidly. At the time of this report the second response is ongoing at 14-20 weeks.
These findings are consistent with the importance of reverse transcriptase in the behavior of the patient’s leukemia and CFS and the potential influence of the clonal T-cells on both these processes. It is possible that inhibiting reverse transcriptase decreased proliferation of both the T and B-cell clones or the effect might be primarily on the clonal T-cells. The rise and fall of cytokines we have documented would be proportional to the absolute number of the clonal T-cells and secondarily could influence the proliferation of the B-cell clone.
Alternative explanations for the therapeutic effect of his anti-retroviral therapy have been considered. One of these is selective toxicity rather than an anti-retroviral effect. Selective toxicity has never before been seen with the hundreds of agents used as cancer therapeutics and seems an unlikely explanation for his improvement especially as the patient had no toxicity at all. AZT, raltegravir and tenofovir have never been shown to have single agent chemotherapy activity so a chemotherapy effect is unlikely to be an explanation. Anti-telomerase activity of the AZT has also been considered, but the rapid response to treatment does not fit the kinetics of depletion of telomeres and induction of apoptosis. Furthermore, an anti-telomerase agent did reach clinical trial and failed to induce remissions. Anti-herpesvirus activity of the antiretroviral regimen is not a tenable explanation of his response as an active herpesvirus infection was ruled out.
There is nothing unique about this patient’s clinical presentation to suggest that his case is any way unrepresentative. His response to anti-retroviral therapy implies that HGRV/MLRVs were etiological for both his CFS and CLL and that anti-retroviral therapy might help other patients with CFS and HGRV/MLRV associated malignancy. Many more patients need to be studied. Ultimately questions that should be answered are what neoplasms are associated with HGRV/MLRVs, will existing anti-retroviral drugs have activity in these neoplasms, will other anti-retroviral drugs such as a protease inhibitor be required and what would be the optimal combination of anti-retroviral drugs.
- Kufe D, Hehlmann R, Spiegelman S: Human sarcomas contain RNA related to the RNA of a mouse leukemia virus. Science 1971, 175:182-185.
- Hehlmann R, Kufe D, Spiegelman S: RNA in human leukemic cells related to the RNA of a mouse leukemia virus. Proc. Nat. Acad. Sci. USA 1972, 69:435-439.
- Hehlmann R, Kufe D, Spiegelman S: Viral-related RNA in Hodgkins’ Disease and other human lymphomas. Proc. Nat. Acad. Sci. USA 1972, 69:1727-1731.
- Kufe D, McGrath IT, Ziegler JL, Spiegelman S: Burkitt’s tumors contain particles encapsulating RNA-instructed DNA polymerase and high molecular weight virus related RNA. Proc. Nat. Acad. Sci. USA 1973, 70:1737-741.
- Baxt WG: Sequences present in both human leukemic cell nuclear DNA and Rauscher Leukemia Virus. Proc. Nat. Acad. Sci. USA 1974, 71:2853-2857.
- Aulakh GS, Gallo RC: Rauscher-leukemia-virus-related sequences in human DNA: Presence in some tissues of some patients with hematopoietic neoplasias and absence in DNA from other tissues. Proc. Nati. Acad. Sci. USA 1977, 74:353-357.
- Urisman A, Molinaro RJ, Fischer N, Plummer SJ, Casey G, Klein EA, Malathi, K, Magi-Galluzzi C, Tubbs RR, Ganem D, Silverman RH, DeRisi JL: Identification of a novel gammaretrovirus in prostate tumors of patients homozygous for R462Q RNASEL variant. PLoS Pathog 2006, 2:e25.
- Lombardi VC, Ruscetti FW, Das Gupta J, Pfost MA, Hagen KS, Peterson DL, Ruscetti SK, Bagni RK, Petrow-Sadowski C, Gold B, Dean M, Silverman RH, Mikovits JA: Detection of an infectious retrovirus, XMRV, in blood cells of patients with Chronic Fatigue Syndrome. Science 2009, 585-589.
- Lombardi VC, Hagen KS, Hunter KW, Diamond JW, Smith-Gagen J, Yang W, Mikovits JA: Xenotropic Murine Leukemia Virus-related Virus-associated Chronic Fatigue Syndrome reveals a distinct inflammatory signature. In vivo 2011, 25: 307-314.
- Levine PH, Fears T R, Cummings P, Hoover RN: Cancer and a fatiguing illness in Northern Nevada-A causal hypothesis. AEP 1998, 8:245-249.
- Matutes E, Taylor GP, Cavenagh J, Pagliuca A, Bareford D, Domingo A, Hamblin M, Kelsey S, Mir N, Reilly JT: Interferon a and zidovudine therapy in adult T-cell leukaemia lymphoma: response and outcome in 15 patients. British J Hematology 2001, 113:779-784.
- Bazarbachi A, Ghez D, Lepelletier Y, Nasr R, de The H, El-Sabban ME, Hermine O: New therapeutic approaches for adult T-cell leukaemia. The Lancet Oncology 2004, 5:664-672.
- Melana SM, Holland JF, Pogo B G-T: Inhibition of cell growth and telomerase activity of breast cancer cells in vitro by 3’-Azido-3”-deoxythmidine. Clinical Cancer Research 1998, 4:693-696.
- Li H, Song T, Xu W, Yu Y, Xin X, Hu D: Effect of 3’-azido-3’-deoxythymidine (AZT) on telomerase activity and proliferation of HO-8910 cell line of ovarian cancer. Int J Biomed Sci 2005, 2:35-41.
- Singh IR, Gorzynski JE, Drobysheva D, Bassit L, Schinazi RF: Raltegravir is a potent inhibitor of XMRV, a virus implicated in prostate cancer and Chronic Fatigue Syndrome. PLoS Pathog 2010, 5:e9948.
- Paprotka T, Venkatachari NJ, Chaipan C, Burdick R, Delviks-Frankenberry KA, Hu W-S, Pathak VK: Inhibition of Xenotropic Murine Leukemia Virus-Related virus by APOBEC3 proteins and antiviral drugs. J of Virology 2010, 84:5719-5729.
- Lee M, Gusho E, Das Gupta J, Klein E, Silverman R: XMRV infection induces host genes that regulate inflammation and cellular physiology [abstract 280]. J Urology 2011, 185(suppl 4):e 113.
- Sciamanna I, Landriscina M, Pittoggi C, Quirino M, Mearelli C, Beraldi R, Mattei E, Serafino A, Cassano A, Sinibaldi-Vallebona P, Garaci E, Barone C, Spadafora C: Inhibition of endogenous reverse transcriptase antagonizes human tumor growth. Oncogene 2005, 24:3923–3931.
- Katz E, Lareef MH, Rassa JC, Grande SM, King LB, Russo J, Ross SR,MonJG: MMTV env encodes an ITAM responsible for transformation of mammary epithelial cells in three-dimensional culture. JEM 2005, 201:431-439.
- Swanson I, Jude BJ, Zhang AR, Pucker A, Smith ZE, Golovkina TV: Sequences within the gag gene of mouse mammary tumor virus needed for mammary gland cell transformation. J Virology 2006, 80:3215–3224.
- Metzger MJ, Holguin CJ, Mendoza R, Miller AD: The prostate cancer-associated human retrovirus XMRV lacks direct transforming activity but can induce low rates of transformation in cultured cells. J Virology 2010, 84: 1874-1880.
- Erdman S., Poutahidis T: Roles for Inflammation and Regulatory T Cells in Colon Cancer. Toxicologic Pathology, 2010, 38: 76-87, 2010.
- van der Kuyl AC, Cornelissen M, Berkhout B: Of mice and men: on the origin of XMRV. Frontiers in Microbiology 2011, 1:1-7.
- Theiler M: Nobel Lecture, December 11, 1951. In Nobel Lectures, Physiology or Medicine 1942-1962, Elsevier Publishing Company; 1964: I:yellow fever Max Theiler – Nobel Lecture.mht
- Rockefeller University: Yellow Fever immunization statistics. In ScienceDaily www.sciencedaily.com/releases/2010/06/100611222839.htm
- Millitary vaccinations. Air Force Joint Instruction 48-110, Army Regulation 40-52, BUMEDINST 6230.15, CGCOMTINST M6230.4E, dated 12 May 2004.
- Koprowski H: Historical aspects of the development of live virus vaccine in poliomyelitis. Brit Med J 1960, 2:85-91.
- Casals J, Olitsky PK, Anslow RO: Adaption of a Lansing strain of poliomyelitis virus to newborn mice. JEM 1951, 94:111-121.
 |
| Figure 1 |
 |
| Figure 2 |
 |
| Figure 3 |
>Hi Dr. Snyderman,
Very interesting. Are you suggesting that we CFS sufferers talk to our physicians about anti-retroviral drugs? What should we suggest?
Also, do you and others studying the disease see a connection between Hodgkins Disease and CFS? In terms of damage to the immune system?
Thanks for your contributions to this important discussion and your information.
>Amazing. Thank you for this work which in my mind is an important step forward.
>I am so glad the meds are helping you Dr. Snyderman. I watch what is going on with you with great interest. You see my brother died from leukemia and I am HGRV positive. A friend of mine also recently died from Leukemia as well. She was diagnosed and was gone within a month. The cancer came on quick and she had no idea how ill she was. Also, My whole family except one brother is ill as well with either cancer or a neuroimmune illness. Two of us have fibromyalgia/ME. I have always been very fearful of cancer after knowing my whole life that that is what took my brother from us. I guess my fears were justified. At least I know how to protect myself and other family members somewhat by having regular cancer check ups. Thank you for sharing your journey through these devastating illnesses, and for being a pioneer in the treatment of them.
>Thank you,both of you, for posting this update, with so much data. A lot of people check this site for exactly this type of information. So many of us are desiring information and rational hope for progress with regards to understanding and treating CFS and problems that statistically seem related to CFS (for example, risks for cancers).
>Dr. Snyderman, thank you for sharing your story so candidly and courageously. I am curious if you have a family history of leukemia, since many of us seem to have related illnesses in our family trees (leukemia runs in my own family, and I have had ME/CFS for almost 20 years). Wishing you continued healing.
>Thank you Dr. Snyderman for sharing your research. Your contribution is appreciated!
>This is an extraordinary effort on your part – both to do all this work, and to share it with us. Thank you so much!
>I'm so glad that you are again responding positively to the RV protocol, and even more glad that you are still with us, Michael Snyderman! Thank you for blazing a treatment trail – all those that come after you will bless your name.
Here's hoping that this encouraging primary data encourages the funding and facilities for a full trial.
As Rabbie Burns might say, long may your lum reek!
>Thank you Dr Snyderman.
Words don't cover how grateful I am that you are willing to do this and speak out about it. We need people to do this to get rid of the politics and let the science speak for itself so that the clinical trials can begin.
>I am a suppoter of Judy Mikovits who has been banned from ME/cfs forums for defending Dr Judys work and I am not the only one.
There are people who are pretending to be supporters of Judy Mikvoits and Frank Ruscettis, when they are clearly not.
I hope people will listen to the scientific analysis at all times and not trust in political statements as the research progresses. This finding is too promising to be dismissed through flawed studies using assays that are not clinically validated.
Tango
>I truly don't understand what this has to do with ME/CFS. Dr. Snyderman…did you have cancer before you developed symptoms similar to CFS? Any kind of cancer would make one severely fatigued, etc., wouldn't it? Or did you have a diagnosed case of ME/CFS before developing cancer?
>Neither do I, but that is the situation. I had hoped the forum was set up for the purpose of discussing science.
Tango
>Thank you for sharing this personal and vital information Dr. Snyderman. It is beneficial for all of us!! It is so important to know how to treat these complex conditions and appreciate you sharing your experience! CFS/ME can manifest in many ways and it affects immune cells and our ability to fight cancer, virus' and bacteria. I have had all of it.
I pray that you get totally well Dr. Snyderman to get back to fully living and working again!
>Shelly,
I welcome your question because it gets into important territory. I had symptoms of CFS long before the cancer. A point I hope to make in the near future is that cancer fatigue and at least part of chemo brain is in reality CFS. The abnormal T-cell clones which Peterson found in his patients with CFS (and cancer) and that I have, are detectable in 40% of my patients with various cancers, not just lymphoid cancers. I have to write up my data but this is a really big deal and my belief (needs research) is that the HGRV causes the T-cell clone and the cytokines/chemokines that the T-cell clone produces can cause some of the pathology in CFS and can also stimulate cancer growth.
Michael Snyderman, MD
>What anti-retroviral medications do you suggest we bring up to our doctors?
Also, do you know of a specific link between CFS and Hodgkins Disease, and do you think that there is a possibility of contagion either way?
Thanks much.
>Thank you, Dr. Snyderman.
Flo
>Kathy d,
I don't feel qualified to give advice on ARVs. I will be trying more ARVs down the line and will post my results.
I believe that HGRVs are involved in many different types of cancer. I don't think they cause the cancer but can raise the level of malignancy. I have a patient who had Hodgkin's Lymphoma as a medical student and at age 45 developed prostate cancer and now has symptoms similar to CFS. Some people would call it Cancer Fatigue but to me it is CFS.
I believe that these viruses are relatively common but some people are more susceptible and research to look at that is being planned by Dr. Enlander. How contagious the virus is would therefore depend on a lot of factors, but we do think it is contagious based on our survey. A larger study will be required to confirm our findings, and we hope that our study will attract support for this.
Michael Snyderman, MD
>Tango is not telling the truth. She is actually V99 and she was talking about Dr. Lipkin on the forum. It had nothing to do with Dr. Mikovits research. She spreads misinformation everywhere and it is harmful to patients. She claims to know science but doesn't have a clue. How would she know how any NIH study should be handled in the US? She is in no way affiliated with science or medicine, or US government in any way. Patients do not want her and her group attacking researchers. Especially those trying to help here in the US. She constantly repeats the same things over and over again hoping people will actually believe her ramblings. She needs to stop as this is hurting patients with this illness.
>Thanks for reporting on this. This is fascinating. Do you find a pattern in the "other" cancers that correlate with T-cell clonal expansion in your patients? ie do they cluster with certain types like prosate, breast, etc.. or is it random?
>FAQ cont.
8. Could these results be due to a placebo response?: Yes
>Thank you for sharing your n=1 results Dr Synderman. I wish many more drs had the guts to at least 'try' ARVs on patients who have no life. I care for one such patient and he would do anything to further the science, even if it killed him. He hates the fact that he has been lying around for 10years + with the whole of medicine ignoring his extreme pain, extreme weakness and fatigue (and more besides). We are alone. Making decisions no patient should be making. I sincerely hope your work is expanded into trials as soon as is possible. Even if the chemo fatigue is realised by drs atleast they'd be vaguely in the loop of what we are talking about. Once again – Thank you
>Anon 11:07
What is wrong with talking about Dr Lipkin? He has been put in charge by Fauci of the NIHs multi lab study has he not? That is having a direct influence on Dr Mikovits and Dr Ruscettis findings.
As patients want transparency and the full design of this study on the NIH website he would have no objections to that would he. Dr Lipkin would want patients keep totally informed on the NIH website, yes?
>"FAQ cont.
8. Could these results be due to a placebo response?: Yes"
Placebo response or placebo affect? What evidence would prove either?
>RE: Lipkin – Assays and study design
This is from wsj
"Lipkin tells the Health Blog that the study focuses on whether XMRV or other viruses in the same family are found in higher frequency in patients with CFS.
As a starting point, everyone had to agree on how to define a CFS patient for the purposes of the study. The issue has been highly contentious and Lipkin says they tried to agree to criteria for patient selection that “includes everyone’s viewpoints.”
The solution: the study will seek to enroll people who in addition to meeting criteria for two widely used, symptom-based definitions of CFS, showed signs of infection — such as a sore throat or tender lymph nodes — around the time they developed CFS. The thought is that if there is a viral link to CFS, it’s most likely to show up in those patients.
More work still needs to be done. The physicians participating in the study will meet with Lipkin in coming weeks to develop a standard checklist for evaluating patients. The scientists are still working out a common protocol for how they handle and process the blood. But Lipkin tells the Health Blog that everything they are doing is designed to make it possible to finally end the debate over whether XMRV is associated with CFS."
The problem is that the items in the checklist and subjective and undefined. The physician is free to interpret the meaning of the terms. If entry criteria are not objectively measurable and constant for every group, i.e. scientific. Then the chance of any definitive findings emerging are remote.
I didnt know that Nancy Klimas is the only physician supplying patients for Dr Lipkins deep sequencing experiments. I am surprised at that because the danger of false negatives are so high. Surely the lipkin study in its entirety should be repeated using ultra deep sequencing and of tissue sampling at that.
Perhaps Dr Lipkin merely suffered from a slip of the tongue.
>Don't worry Ian Lipkin is not looking for XMRV
Dr Lipkin is a supremely intelligent man and he knows that XMRV is a laboratory artefact. He would not look for a laboratory artifact in the blood of people with ME. He knows full well that the viruses found in the blood of people with ME are PMRVs and will not let anyone optimise their assays using the VP-62 sequence which we know does not exist outside a lab. If anyone is still worried I'm sure that Dr lipkin will reassure them. He has the welfare of people with ME at heart and he is very accessible by e mail.
The trouble with an expert virus hunter like Dr Lipkin is that he probably expects others to be competent. Given Mr Switzer's less than impressive collaboration with Dr Sattesfield thus far he will probably supervise the CDC effort very closely and ensure that Dr Lo uses the correct assay.
>One argument for contamination that can easily be knocked down is the sequence diversity of human gamma retroviruses.
Coffin and Towers claimed little sequence diversity is evidence of contamination.
If you go to this link and scroll to image on slide number 5, you can see there are two ways a retrovirus can replicate. Mitotic division leads to little diversity and is established as the method used by gamma retroviruses in mice.
http://idrn.org/documents/events/presentations/Bangham,%20Charles.pdf
>Thank you so much Dr. Snyderman for sharing your one person experience with the community and the world. You are very brave. Brave for all of us not just yourself.
I am hoping you will be able to get your virus sequenced? Any luck in that area? Maybe you can't say but I hope it happens.
Keith
>Keith,
I am happy to have your question. Dr.Mikovits sent samples to two different laboratories, one in Canada to do the integration study and one in California for deep sequencing.
Indeed an integrated virus was detected, integrated at a site unlike where XMRV integrates. To prove this was not due to contamination, I sent a fresh sample and libraries have been made (I don't understand the technical aspects) and will be sent out in a week to a third laboratory for the actual integration studies. The sample for deep sequencing was received about 5 months ago but hasn't been processed and an offer for a fresh specimen was declined.
So we will have integration data back soon to confirm the initial positive results. I am offering fresh samples to any of the scientists reading this blog for deep sequencing. Actually I am CHALLENGING the scientists who are sure that the virus doesn't exist to do the deep sequencing. I have 5 liters to give to the cause.
Michael Snyderman, MD
>Anon@3.52
The point is that a one person trial cannot prove whether the positive results are due to ARVs, the placebo effect or some other factor. It's meaningless.
A friend of my sister's with advanced pancreatic cancer was told she had days left a few months ago, but after a few sessions of reiki she was up and about and is now doing much better. This does not prove that reiki can effectively treat cancer. It proves nothing, but is a wonderful and amazing thing for her and her friends and family, just as Dr Snyderman's improvement is a wonderful thing for him and his loved ones and long may it continue….
>Dr. Snyderman, what do you think of the following public comments by a prominent CFIDS physician?
"There is still no consensus in either direction for the existence or non-existence of XMRV associated with CFS cases. Studies out of Europe (Belgium and Germany) and the US (Cornell) as well as elsewhere which are separate from WPI, FDA and NCI are demonstrating evidence that cannot be due to a mouse contaminant for XMRV association with CFS. The strongest supportive study to date was reported by Dr. David Strayer out of Hemispherex Inc, (Philadephia, PA) at IACFS/ME in Ottawa and showed that 7/8 CFS cases and 2/17 controls were positive for XMRV using Next Generation Sequencing (NGS) technology available at Roche Labs in Germany. NGS is not susceptible to mouse contamination and demonstrates that XMRV is in fact integrated into human DNA which means it is a human virus. The Science (Lombardi et al, 2009) study still stands as the best evidence that this virus is transmissible from cell to cell and the studies out of WPI and Belgium demonstrate an immune response (antibodies) to XMRV and a cytokine profile (WPI) that suggests it is pathologic.
I expect that Next Generation Sequencing or NGS, which does not have the flaws of PCR technology in evaluating a poorly understood human virus(es), will be the best way forward to a consensus as to the question of association of CFS with XMRV/HGRV. This preliminary report out of Germany using NGS as well as human immune response data supports the association of XMRV with CFS, despite the flaws exposed in the current primary PCR technology used to define this scientific debate which appears very messy and excessively bio-political to date."
There's no question that next generation deep sequencing studies are desperately needed on TISSUE, not just serum. Are there less toxic ways of mitigating the upregulated cytokine pathology you describe besides ARVs, assuming cancer is not present?
>Placebo effect is usually shortlived, maybe a couple of weeks or so. It does not last 17 months, particularly in the case of cancer. The most difficult disease to study regarding placebo effect is not cancer but migraine headaches where the placebo often outworks the drug being tested. This makes sense because migraines go away and return without any clear reason as to what is going on. Perhaps increasing "feel good hormones" which a placebo might affect explains it. Placebo would not explain reduction in measurable indications of cancer.
But y'all can google this stuff yourselves.
>Excellent and important stuff.
>Michael's paper, that is.
>@Paula
Nobody knows how the placebo effect works, but it undoubtedly does. There a thousands of placebo controlled cancer drug studies showing measurable improvements in 10-40% of the patients given placebo. Fact. I would suggest pubmed or google scholar if you want proof. Pretty much any large scale cancer treatment study proves it.
The placebo effect is not imagined, but real and measurable. In fact there have been studies where the placebo group on chemo drug trials have experienced hair loss, because they had been told it was a possible side effect. Placebo effects can be lasting and many have experienced lasting remission of cancer and other diseases.
>For anybody interested in learning a little about the power of placebo. Very interesting documentary:
Placebo: Cracking The Code (Parts 1&2)
http://video.google.com/videoplay?docid=4115610193400691959
http://video.google.co.uk/videoplay?docid=-6942125248944933588
>Regarding placebo, nobody has made a claw for me yet.
>I am not willing to debate something as vague as placebo being the fix for Dr. Snyderman. Anything is possible but highly unlikely over a period of months. Of course, we cannot conclude from his case that we all should jump on the bandwagon of ARVs. Real science identifying retroviruses and then testing a lot of patients for effective treatments will be the answer we seek.
Check out this link:
http://www.quackwatch.com/04ConsumerEducation/placebo.html
"On rare occasions, even cancer can inexplicably disappear (although most testimonials for quack cancer remedies are based on faulty original diagnosis or simultaneous administration of effective treatment)."
It certainly does not indicate that placebo effect cures 1 of 3 cancer patients.
>I doubt this about placebos and cancer. I've seen too many people very sick with cancer, including young people with everything else in their lives going well, but they got cancer.
Fast-growing, very lethal cancers are not easy to beat, although there are treatments now which can cause remissions. But it is a battle, and it's not always won.
I would not put out into cyberspace that people with cancer don't need treatment that's been shown to help beat back the disease.
People can always try leeches and bloodletting, or copper bracelets, but they won't stop cancer cells.
Cancer is ruthless. Why not promote the best treatments?
>Anon 12:48,
Unfortunately, I have to disagree with you on this. Placebo arms on controlled drug studies for cancer do not show objective response of the cancer. There are a lot of phase 1 and phase 2 trials where there were zero response to experimental cancer drugs and if there was a placebo effect, objective response should have been seen. With respect to myself, I was doubtful that the ARVs would work and was pleasantly surprised (to say the least) when they did. Therefore, that could not be a placebo, mind over matter response. I do, however, recommend that we all keep a hopeful and positive attitude.
Michael Snyderman, MD
>Dr Snyderman
Thank you for answering my question.
Thanks for continueing yor efforts!
Keith
>Well, I've seen people beat back terrible cancers with surgery, chemotherapy and radiation, diseases that 20-30 years ago had a very low survival rate.
Or friends who went into remission for years after treatments for horrific diseases.
>@anon December 17, 2011 3:50 That's not the point. Tango aka V99 said mecfsforums was banning patients for supporting Judy Mikovits. She was lying. That forum has always fully supportive of Dr. Mikovits and always will. But there is something very wrong with Tango/V99 bashing every scientist and doctor who tries to help with this illness. But it appears she has since changed her postion as "It's a mouse" on People with ME forum. I guess she has finally come to her senses and realizes there are some that actually want to help us. Let's leave the science to the real scientists. The Lipkin study is listed on the NIH website. Just have to look for it.
>The message directed at anon December 17, 2011 3:50 was actually meant as a response to anon December 17, 2011 3:35am.
>This is why the Anonymous label is confusing. One never knows whom one is responding to, if an Anonymous has changed his/her position, which of several positions is a particular Anonymous defending or refuting. I've given up on the Anonymi.
>dr. s,
thank you for being such a brave pioneer — and a good writer to boot.
rivka
>Thank you for being brave enough to continue your important research and to post information about it publicly, Dr Snyderman.
If your ideas are correct they must necesarily lead to a massive shift in medical paradigms, and this makes all the outcry against Dr Mikovits and Dr Ruscetti's work comprehensible, if regrettable.
If the implications of this research and the mistakes of the past can be courageously faced, however, it offers exciting new opportunities for the treatment of cancers and other intractable disease. Thankyou for your bravery in trying to bring this change about.
>The full details of the Lipkin study are not on the NIH site.
"and this makes all the outcry against Dr Mikovits and Dr Ruscetti's work comprehensible, if regrettable."
It really doesn't
>Thank you Dr Snyderman for sharing this important information with us. I wish you the best of possible outcomes.
I'm wondering if you know whether you suffer mytochondrial damage from using AZT and whether that sort of damage should be of high concern to those of us who have had CFS/ME for decades and don't have a lot of time left to "wait and see" what develops. Is there a test for this kind of damage or do you just monitor your liver and kidney functions?
My vaccination history parallels yours: oral polio in late 50s or early 60s, yellow fever vaccine in 1972. Then struck down by a "killer flu" in 1982 and downhill ever since. Disabled since 1/1989.
I'd like to try AZT but I'm undecided about the risk/benefit ratio.
-Oerganix
>Myhills mitochondria test can measure the damage, which will probably exist as a result of a HGRV infection.
>Good Discussion going on guys. Carry on. I learn so many good things from blog as well as from discussion. Thanks for sharing and carry on discussion to share more.