
The intrepid Dr. Mikovits went up against Darth Vader today in Ottawa. In the face of incredible adversity, she took the heat. For us. And she points the way to the next step. Next Generation Sequencing. Here are her slides. Click each to enlarge. May the force be with her. Brava!






















>@Jill Neimark
EBV and other herpes virus hypothesis have been investigated and thrown up nothing. Not every patient is infected with these and they are not known to cause such symptoms and biomedical abnormalities as those present in people with ME/CFS. A hypothesis requires that you have a proposal that is testable. There is none left for these pathogens, whereas for HGRVs the hypothesis is easily testable and now confirmed in 3 separate studies.
HIV is not a usual retrovirus, in fact it would be best described as the odd man out. The properties of HGRVs are no different to other gamma retroviruses. The story is no different for Beta and Delta retroviruses. HTLV also provides a better picture for comparison and as Mikovits has pointed out has 1% genetic alteration in 1000 years.
>Now that I've worked out how to use this thing, I'd like to thank both Jamie and Dr Snyderman for being courageous enough to make public the details of their illnesses and treatment.
It has been most encouraging and interesting for me to follow, but I appreciate that it cannot always be easy for you when it entails opening yourselves and your private concerns and decisions to criticism from unknown posters.
Best wishes and good health to you both!
>Jill,
I very much appreciated your comment about the characteristics of antiretrovirals (directly immunomodulatory, affect apoptosis, affect t-cells, directly anti parasitical). Insofar as we are going to defend the usage of ARV's in this population, having as many explanations as possible about how they might be working apart from their activity on retroviruses is helpful at this point.
I'm far from an expert on retroviruses, so I don't know the answer to the question about how quickly a retrovirus like XMRV might rebound after the drugs are stopped.
It certainly is the case that some patients who get improvements from herpes antivirals (e.g. Valcyte, Vistide) do maintain those gains for at least a while after the drugs are stopped though. I stopped my own herpes drug "cocktail" (Valcyte and Famvir) about eight months ago and have experienced only further gains since that time.
Quite frankly, I think it's possible to make a case that my own recovery (to close to full wellness, apart from some mild tiredness and some residual moderate biotoxin reactivity) followed precisely the same path as Jamie's: move to a different location, aggressively pursue detox (including methylation); take drugs that target herpes viruses (in her case, Raltegravir); tinker with the hormones; support the system.
Do I know that's the case? Absolutely not.
But it's an alternative hypothesis that (in light of the current state of the knowledge on XMRV) might at least be considered.
Best, Lisa
>Muckle, my questions are important, and none of them have been addressed sufficiently, if at all. — Jill
>@ Gerwyn/Muckle,
The reason I got the 3,7% from WPI, is (of course) because that was the incidence they were finding it with. Even if there is an incidence of 14%, their assays are apparently not able to detect all members of the HGRV family. And as your argument hinges on the idea that WPI could not reliably detect all HGRV's using these assays, there is no reason to go with the highest possible percentage out there.
I was even rather generous, as Mikovits and Ruscetti actually found the virus in 12 out of those 15 people. However, unlike you, Ruscetti knows his assay is not "clinically validated" and din't count 1/3 positive result as being positive.
But hey, let's recalculate with the 14% from that Belgium guy. Then the odds of this "11 out 15 positive" event happing are then "only" 3 out of 10 million.
Oh, and I see you want to eliminate the lab workers as well, as they were not completely randomly chosen. With a 14% chance of being positive, the chances of selecting 9 out of 12 blood controls to be positive for this family of viruses are 3 in a million.
I see you have completely invalidated my argument with that. ;-)
In line with what Ed rightfully argued, these disastrous results really only leave two options:
– WPI's results are clearly wrong
– Conspiracy
And of course, with a conspiracy, the question then remains how the conspirators could find all those positives with "unvalidated assays" and managed to get these positives through the WPI and Ruscetti labs without them noticing.
However, there is no way in actual reality that these results can be explained away with any of the supposed shortcomings of the BWG study that were proposed in this thread.
>jill activated microglia would lead to a neutrinflammatory disease and mitochondrial damage.
These are the inducers of pathology in other neuroinflammatory disease and neurodegenerative ones. If you want the mechanisms involved I would be happy to supply them
grvs activate microglia and cause mitochondrial damage.it is very well documented
the cytokine pattern of people with ME precludes the involvement of EBV as a causative agent.This has been investigated many times
grvs are well known to cause neuroimmune pathology in Apes cats and mice
HIV replicates almost exclusively via reverse transcriptase but other genera of retroviruses dont.Clonal expansion is a very common mode amoung gammaretroviruses and delta retroviruses replicate by almost exclusive use of this mechanism and pathology is related to aberrant viral proteins.This phenomenen is also observed in gammaretroviruses where neurotoxicity is caused by misfolded env proteins
>Here's an excellent video in which Stanford's Jose Montoya talks about his experiences using herpes antivirals in his CFS patient base.
http://www.youtube.com/watch?v=Riybtt6SChU
I also like this comment of his from the video.
“One day, my dream is our medical community will produce a formal apology to the patients for not having believed them all these years that they were facing a real illness.”
I think it's hard for anyone to make a case that he's not on our (the patients') side.
Best, Lisa
>As for the retroviral hypothesis, my CD4 and CD8 counts were depleted very early in the course of illness. I had ARC (AIDS-related complex) some two years into my illness. My NK and CD4 counts remain low, despite many clinically sucessful treatments and generally feeling better. EBV, mold, VOCs, and any other number of "co-factors" probably contribute to precipitating illness, but there is something sinister, clever, and infectious that underlies this illness. My wife caught it from me and now my daughter is showing signs. EBV does not behave in that manner, whereby the body doesn't clear it without something more nefarious onboard. HHV6a might be capable of exacerbating the destruction of T-cells, but nothing besides a retrovirus is capable of depleting CD4 and/or CD8 cells, as well as NK cells, aside from ablation or exposure to radiation or certain poisons. Mold is incapable of doing this to CD4 cells, though I'm sure it piles on.
As for the Lipkin/BWG studies, what a mess. So many arbitrary parameters, so much lack of control for factors that could obfuscate the results, such a poor choice of patient cohorts in that some doctors' patients (generally the sickest with a particular pathological cytokine profile) were excluded from the study. Anyone defending the study as "science," doesn't understand science. And who's to say the NIH didn't somehow botch the code (inadvertently or deliberately through their outsourcing)? This is all just so sad. Unfortunately, given the precarious position of the US economy and the fact that it's about to get much worse, the government can't afford another epidemic.
For those of us with infectious onset and a severely depleted immune system, followed by innate immune exhaustion, this has all the hallmarks of a retrovirus, whatever frigging name you want to give it. Judy's conclusion about deep sequencing finding retroviral fragments in the circulating nucleic acids from apoptotic cells in CFS (M.E.) patients should've raised an eyebrow from all of you.
I am not advocating the use of ARVs, because I think they are as toxic as they are "immunomodulatory," and most of the literature bears that out. However, I respect an individual patient's decision to employ them lacking any other proven or effective therapy.
Sincerely,
A disgusted former microbiologist.
>Gerwyn (this sounds like Gerwyn anyway!) wrote:
>The cytokine pattern of people with ME precludes the involvement of EBV as a causative agent. This has been investigated many times.
I don't think anybody's suggesting that any of the herpes viruses is a causative agent. That was the first explanation suggested in 1984 ("Chronic EBV"), and it was eliminated almost immediately thereafter.
Clearly, the herpes virus infections are opportunistic to something else (which could be XMRV or could still be a mystery). With the NKC dysfunction that we have, it would be a miracle if we didn't have problems with herpes viruses.
The point is that even though these bugs are opportunistic, they may be serving as a "progression factor" that makes our condition much worse.
Possibly, the hypothesis goes, the reversal of this progression factor may have the potential of explaining the case histories of the doctors using ARV's that have been reported on this blog.
Best, Lisa
>>HHV6a might be capable of exacerbating the destruction of T-cells, but nothing besides a retrovirus is capable of depleting CD4 and/or CD8 cells, as well as NK cells, aside from ablation or exposure to radiation or certain poisons. Mold is incapable of doing this to CD4 cells, though I'm sure it piles on.
Speaking of radiation, here is an interesting hypothesis related to our illness that discusses just that.
http://cfsuntied.com/blog2/2011/09/15/and-now-for-something-completely-different/
Unfortunately, I don't have enough scientific knowledge to evaluate this theory in the way that I would like. I thus would very much appreciate comments from the scientists or other obviously very smart people reading this blog.
Thank you very much for your help.
Best,
Lisa
lisapetrison at yahoo
>Gerwyn and Muckle – this seems to be very important information and I'd like to know more. But its a bit hard to follow when bits of information are added here and there. Is it possible for you two to get together and put all of this story together so that we can see the situation and the problem laid out clearly?
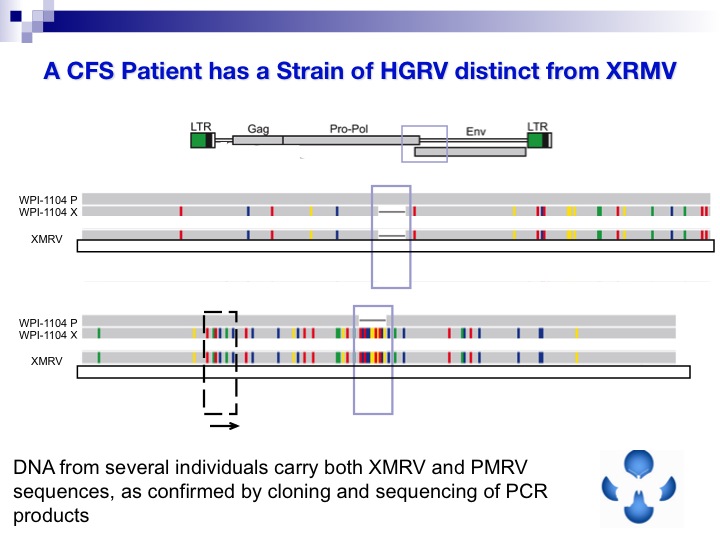
When Silverman discovered GRVs or MLVs in prostate cancer in 2006 did he knowingly create the false VP62 clone which has lead to all this misunderstanding? Why did WPI originally know to make a VP35 and not VP62 and why was this critical information missed by everyone? When was the problem with VP62 discovered? Shouldn't Sivlerman's research and paper now be corrected? Why didn't the WPI or BWG know about the problem with VP62 as well as the other problems with preserving etc?
BTW I'm confused about whether these Viral Proteins are from a fully sequenced gammaretrovirus and why particular proteins are chosen and should many different proteins be used to find the variations?
Sorry if my questions don't make sense, I'm just so sick and struggling to understand the whole story, which I suspect is very significant reading Coffin's reaction to the mention of a connection with Autism and this dodgy science & psychiatry negative PR campaign to discredit neuro-immune diseases and GRVs.
I hope you can find a way to do this, it seems there is a lot at stake here and we need to be armed with all the facts to analyse the situation and plan how to counteract the attacks against us and the science, our lives and our human rights depend on it.
Thanks Jamie for your continued presence and reassurance in sharing your thoughts with us, it means a lot to know who our friends are in this battle for the truth against the big big lies!
XRxfan
>the vp-62 clone is a composite made from different patient,s tissues
the primers originally used by silverman were based on vp-35
dr mikovits and dr Ruscetti lowered the annealing temperatures and increased the magnesium concentration in their PCR to increase sensitivity and this is why they picked up the entire community of gammaretroviruses present in the cohort
They could not detect env sequences because the env primers could only pick up vp-62 and they were too different even for the lower annealing temperatures to detect
the VP-62 clone does not exist in nature so all the 00 studies which set their PCR to detect the synthetic VP-62 clone would have no hope of detecting a real virus
The interesting point is how does john coffin now explain how he demonstrated that two gammaretroviruses recombined to form an artificial clone which does not exist in nature when one of those gammaretroviruses has not been demonstrated to exist in nature either
>Dear disgusted microbiologist,
In all sincerity I obviously do not know the entire viral literature, but are you suggesting only a retrovirus would target CD4 and CD8 cells–and that this yet unidentified one has targetted both of yours?
When I wrote about HIV, I learned a little bit about it, and that it uses the CD4 receptor, along with a secondary receptor (ccr5 or cx4, I believe the other is called). It binds to the receptor(s) and has to turn to get in. So for instance Lo's lab is now working on an antibody that blocks part of the CD4 receptor, enough to allow it to function but also to block that turning mechanism thus preventing HIV from entering.
Are you suggesting that there is a retrovirus adapted to target primarily two different receptors on two different immune cells? How would that work.
I'd like to understand that. As at first glance that sounds quite perplexing.
And you are saying that no other entity, virus, fungus, or bacteria of any kind, can damage the CD4 and CD8 cells?
Thanks
Jill
>@RRM
You are now speaking to Muckle.
With any pathogen assays are improved upon in the hope they identify everyone infected. To argue that the first assays used for detecting virus in blood should produce gold standard levels off testing when our understanding of HGRVs is very rudimentary is foolish.
This is how I replied to your opinions earlier.
"You are jumping to conclusions. We have no idea where those people were from. They could all be positive. They were also not randomly picked.
Lombardi et al. found 4% positive. Lo found 7%. There is a paper circulating that is finding 14%. As techniques improve the numbers will increase, with some areas having a higher concentration of infected and others lower. HIV and HTLV are no different.
You are mistaken in thinking you have applied any calculation and your opinion is merely speculation."
At no time did I "to go with the highest possible percentage out there." It was to illustrate how speculation such as yours serves no one. We don't know if the controls would have been found negative if all labs had been given the privilege of screening them.
You are incorrect about Ruscetti's assays also. They are fully validated. It was the people running the group that stimulated that samples must be positive multiple times. Again, this is a foolish position to take when little is understood about the pathogen in question.
It is plain that not all labs were provided with the controls to screen, thereby invalidating the paper. The failure to use Trizol or an equivalent is also invalidates the paper. I'm certain this is not what Busch set out to achieve. I think it is important that you don't start accusing such people of a conspiracy RRM, you are being rather unfair. We have no idea of the pressure such people are under.
>To Former Microbiologist –
I do hope you'll take a look at the link in my last post and (if you would) consider sharing it with Dr. Cheney. I've respected your opinions since our discussions a while back on ProHealth, and thus would like to know if you think the hypothesis posed is plausible.
I do think we have to be careful with this disease when we use words like "caught." Just because people in close proximity to one another get the same disease does not mean that it is caused by a pathogen.
For instance, people who live in close proximity are exposed to the same toxins, and those who are related by blood share the same genetics (including, conceivably, the ability or inability to eliminate those toxins from the system).
It also may be that toxins are passed from mother to child in the womb, meaning that children can be born with a high toxic load without ever being exposed themselves. If that's the case, then a relatively small amount of additional toxic exposure as they progress in life may be enough to tip them over the edge into disease at an early age.
As I said, I'm not discounting the idea that a retrovirus is playing a role in this illness and actually think that the phenomenon is better explained by including a retrovirus than by leaving it out.
I'm just trying to present as many different plausible hypotheses as possible with regard to what is going on, so that we have a better chance of getting to the truth.
Thank you very much in advance for taking a look at that link. I am looking forward to your comments.
Best regards,
Lisa
>@XRxfan
There is little of this that will have escaped the attention of relevant parities, but as always I will always endeavour to pass on these concerns to others.
The seminal paper from Silverman in 06 used VP35 for the RT-PCR assay that screened all patients. This was the basis for the assay used in Lombardi and Lo, with minor modifications to account for a blood based gammaretrovirus assay rather than tissue. This detail is within Lombardi et al. (2009) and Urisman et a. (2006) if any wishes to check.
The only full clone of the virus in prostate cancer is VP42.
>Jill, while we may be talking about a whole host of HGRVs, XMRV tropism is specifically geared toward the XPR1 receptor, which is ubiquitously expressed on all mammalian T-cells. These "other" viruses may have other routes of entry. HHV6a has been demonstrated in some studies to be an efficient killer of CD4 cells, and many have postulated it as a co-factor in AIDS progression. I am admittedly not well-versed in ALL of the microbial literature, but to my knowledge, no other pathogen, other than in the role as a co-factor, can deplete CD4 or CD8 cells to the extent that a retrovirus can. Again, that's controlling for a lack of exposure to other poisons or radiation.
Lisa, I do believe you have many pieces of the puzzle. I also believe genetics and toxins may exacerbate susceptibility. However, all of my siblings and my father got sick in different environments (though, admittedly, they could've all been toxic), and my wife's genetics are very dissimilar to my own, and she got ill in an entirely different environment altogether after sexual exposure. My daughter is in an entirely different and mostly pristine environment atogether. All of this has the signature of an infectious pathogen.
FWIW, I've attempted to control my environment to a certain extent, going to the "erythropoeitin heights," as well as camping outdoors, but have never experienced a noticeable and sustained alleviation of symptoms. I don't want to make this about mold, even though I believe a certain subset is more susceptible here.
Disabled and disgruntled.
>scientific hypotheses are explanatory models of empirical objectively measured phenomena
Ahything else may be called a hypothesis but from a scientific perspective it is speculation
Thus far a family of gammaretroviruses have been detected in patients with ME
These retroviruses cause neuroinflammation and mitochondrial damage in other species
thus the hypothesis that grvs cause ME is a plausible parsimonious consilient hypothesis
there are no other scientific hypotheses to consider
>Having said that, I've achieved a KPS score of 70+ employing methods that are a 180' of those suggested on this blog. I ebb and flow like everyone, but I am functional most days.
disgruntled.
>Gerwyn, you are correct sir.
disgruntled.
>Jill,
I am aware of the study you mention. The goal was to destroy all B-cells both benign and malignant which in my mind is not a good thing to do. Patients will have all sorts of horrible infections including multifocal leukoencephalopathy which is seen with rituximab. Also they used an HIV derivative to transfer information to the T-cells, again this doesn't sound like a good thing to do.
Please read my previous letters re: clonal gamma delta T-cell expansion. This is the connection with the immune system and CFS and cancer.
One of the requirements for premed courses is solid geometry. You learn the following logic: identify ALL possible explanations for the data and then eliminate as many as possible. The one left standing is your explanation and that is sometimes what we have to do in medicine and it works. Please read my prior posts. You will see that the only plausible explanation left standing for my personal data is a HGRV. In fact, my plasma was sent out to a reference lab equipped to do the new generation of testing that Dr.Mikovits would like to use and the plasma was positive for Gag RNA.
You have said a number of negative personal things in your comments and that, by the way, hurts your credibility.
Michael Snyderman, MD
>Lisa, I have to sign off, but I'm going to try to reach out to you at some point. I should semi-retract my comment about doing a 180 from suggestions on this blog. I haven't employed many of them, but I don't agree with some of what's been put forth about oxygen (based on experience) or certain sleep meds, some of which can be neuroprotective and immunomodulatory in their own right. However, my primary lingering "clinical" issue is, in fact, sleep, and I think neurofeedback can prove invaluable there, so I hope Dr. Decker-Jones, who I have tremendous respect for, will put up a blog on it.
microbiologist
disgruntled.
>Jill,
As I said on FB, the tone of your question/comment is so disrespectful that it is almost unworthy of response. I'm sure, when a blog forms, I will put it out there, because that's what I do, not because I owe you, or anyone, any explanations.
And pretty much everything you've asked is addressed somewhere on the blog. You're the only person complaining that I've been holding back:).
AZTand tenofovir are immunotoxic. The PI's have immunomodulatory benefits, as well as significant metabolic costs, but they are not yet involved in this discussion.
Jamie
>I think another point worth mentioning is that grvs infect and integrate into CD20 B cells
destroying such cells gives some relief of symptoms but once the use of the monoclonal antibody stops the symptoms return. This would be expected if a grv infected progenitor cells in the marrow and homeostatic mechanisms engage to restore the CD20 B cell population
>I think I'm in love with Ed and RRM.
Seriously. Thank you for helping me put this issue to rest. Your arguments make complete sense to me. I disagree with Gerwyn's pronoucement that "there are no other scientific hypotheses to consider", when in fact there are many, and they're (almost) all in the CCC definition criteria.
And thank you Jamie, for allowing open discussion. I'm very grateful.
>at robin name another scientific hypothesis that explains the symptom spectrum of ME
>And significantly increases the risk of leukemia in first degree relatives (chi-square significant on first pass, small data set).
>Dr. Snyderman–
No, only a small portion of B cells die, I want to say about 1% are infected longterm, but that's from memory from several years ago and might be wrong. Not all B cells are infected with EBV.
There was no immune suppression. So I'm not sure what study you are speaking of. This guy was doing great, with two injections, and completely side-effect free except for a weal at the site of injection. He had complete remission. His only sequaelae were from the draconian chemo treatments…previously.
I do not know whether he has relapsed, could relapse soon etc.
There were lung cancer patients also in complete remission I spoke with. A pancreatic cancer patient with just a few months to live was given a new lease on life but that is so deadly that I assume that was only a partial remission.
This is all Malcolm Brenner's work. It's quite remarkable. Stunning actually.
As to credibility–questions are either valid or not.
Jill
>Jamie, this is what you wrote a few days ago,
"I went down for a while after I wrote the last blog. I was feeling poorly and it was coloring my outlook, so I didn't want to write anything I'd regret."
What does that mean? What constitutes a dip? Why not speak about dips? What would you regret? Do you only write when you're feeling better now? Is that an honest appraisal?
Hey, you can write whatever you want…but it raises questions.
Then you wrote:
"When I felt myself dip, I stopped Isentress, because experience has taught me that when things are going south, stop what you can."
I have no idea what that means. Stop what you can? How do you know what you can stop? Why did you choose to stop a seemingly life-altering drug (one that got you out of bed supposedly).
"I was all over the place at the time, but didn't notice anything I would call better or worse from stopping the drug."
So what does that mean? Is your retrovirus latent now? Did your year of treatment put it into latency and you can stay off until you dip again?
The whole thing is, as you say, all over the map.
Makes no sense.
If it is disrespectful to question this, so be it.
>@Muckle
Ruscetti designated two patients and one control as being "UNDETERMINATE" for HGRV positivity based on his serology test. He did this because these samples gave only one positive out of three times tested. This logically proves that Ruscetti does not regard his single serology test using the Lombardi et al.'s methodology as "fully validated". After all, he then would have designated these patients/control as "positive".
– I am not speculating. The odds of finding 11 out of 15 controls that were pedigreed beforehand BY ALL LABS that claim to be able to detect these HGRV's, are astronomically low.
I was merely showing that these odds are atronomically low, by calculating the odds with an example that basically had each possible variable in the HGRV proponents' favor. That is not speculating, but rather illustrating that the used argument is invalid.
On the other hand, the sheer amount of speculation you would have to undertake to reach any reasonable explanation for finding 11 out of 15 pedigreed negative controls to be actually positive for HGRV's, is beyond me.
– You are misrepresenting the pedigreeing that was done. ALL samples were sent to Lo/Mikovits and Ruscetti (as well as two "negative" labs), and all of them agreed that ALL samples were negative using their own, self-chosen assays.
Furthermore, ALL of the labs that weren't involved with the pedigreeing of negative controls, ALL agreed that all control samples were in fact negative. Just check the study results!
(BTW: I did not intent to imply that you and Gerwyn were the same person. It is actually very easy to see that you are not the same person. I was just responding to both your posts, but I agree that I was no entirely clear with that. Sorry about that.)
>Jill,
I experienced an exacerbation of symptoms for a couple of weeks, after a period of great stress. As can happen with this disease, my mood was affected, and I thought it might be coloring my judgement.
I went off Isentress as a wash out, planning to start AZT or Lexiva again, probably the latter. I want to get baseline labs before doing anything else, but have to go back to Santa Fe to do that. I'm taking the red eye home tonight.
I think most ME patients know what being all over the place means:).
I believe that we were helped by arv's, but I can't prove it. As I've said many times, I could be wrong about anything. I share because there is an information vacuum with respect to treatment. Not because I'm trying to prove anything to anybody. I DON'T KNOW.
When we started arv's, I thought there would be viral load measures available soon. Now it is all guess work. There is nothing to monitor like Dr. Snyderman's CLL. It clearly isn't like treating HIV. On FB, you mentioned our resorting to 20 year old CAM therapies. Things seem to be working for us now that didn't work before. But people write to me who got better for no reason at all.
My instinct, coupled with a very small amount of anecdotal information, the experience of under 50 patients, completely uncontrolled, is that I don't want to give up arv's, especially Viread. I think my reasons go beyond the satisfaction of civil disobedience. It is completely crazy that the off-label use of these particular, not very dangerous drugs has risen to this level of furor, though that seems to be par for the course when someone actually tries to treat these most difficult of patients.
Jamie
>@RRM
The people running the blood working group interpreted positives as intermediate, not Ruscetti. Not all labs screened all controls and none were pedigreed. This is made very clear in the paper. It does help if you have received appropriate training when you sit down to read a paper.
It was a curtsy to you that I make it clear who you were conversing with as I could tell you were struggling reading.
>RRM
The paper definitely doesn't say everyone was looked at by all the labs.
>Not all the labs within the BWG did screen the controls, that is correct. 44,654 labs outside of the BWG did also no to that. Do you know why? Because of economic/efficient/time reasons, you pick the labs that have the most chance of "catching" some healthy positives. And just as those 44,654 other labs not validatig the controls does not invalidate the results, the lack testing by a couple of labs that never had detected "wild type XMRV" anyway doesn't.
To rephrase: ALL of the labs that claimed to have "VALIDATED" asays, as well as two "negative" labs, pedigreed ALL of the negative samples. That means that WPI pedigreed all negative controls, Lo did pedigree all controls and Ruscetti did pedigree all controls, as well as the Switzer and Coffin labs. Why would that not be enough?
If you're still not convinced, suppose that just those same five labs would test them after pedigreeing. I understand that then, those same five labs doing the pedigreeing would heve been good enough for you? Do you realize how scientifically flawed this line of reasoning is? After all, five labs pedigreeing in a seven lab study is just as good as those same five labs pedigreeing in a three lab study.
Now, with regard to all this pedigreeing done by labs with supposedly validated assays, there is NO WAY in actual reality that 11 out of 15 (or 9 out of 12) of those WELL PEDIGREED negatives happened to be positive.
BTW, ironically, it seems you are the one with some trouble reading. The participating labs themselves decided when to call a result as "intermediate" and not 'the people running the BWG' (who are 'the people running the BWG anyway and how would they decide? By popular vote?). But thanks for the *courtesy*.
@Anonymous September 25, 2011 5:46 PM
Duwing pedigreeing that would be correct and that is why I didn't say that either. Fact is however, that Lo, Mikovits and Ruscetti (as well as Coffin and Switzer) did pedigree ALL those samples with whatver methods they prefered and that ALL five labs agreed that ALL 15 controls were negative.
>The only people that are said to have been screened by all labs, and still not called pedigreed, are 3 lab controls. Can you not read?
>Yes, I can read, thank you very much.
To check if you can read, could you please quote a passage where I have stated that all labs had checked all of the controls?
>Good you are owning up now
>Now, now, play nice. We all have to play in the same sandbox.
ALL I REALLY NEED TO KNOW I LEARNED IN KINDERGARTEN
(a guide for Global Leadership)
All I really need to know about how to live and what to do and how to be I learned in kindergarten. Wisdom was not at the top of the graduate school mountain, but there in the sand pile at school.
These are the things I learned:
Share everything.
Play fair.
Don't hit people.
Put things back where you found them.
Clean up your own mess.
Don't take things that aren't yours.
Say you're sorry when you hurt somebody.
Wash your hands before you eat.
Flush.
Warm cookies and cold milk are good for you.
Live a balanced life – learn some and think some and draw and paint and sing and dance and play and work every day some.
Take a nap every afternoon.
When you go out in the world, watch out for traffic, hold hands and stick together.
Be aware of wonder. Remember the little seed in the Styrofoam cup: the roots go down and the plant goes up and nobody really knows how or why, but we are all like that.
Goldfish and hamsters and white mice and even the little seed in the Styrofoam cup – they all die. So do we.
And then remember the Dick-and-Jane books and the first word you learned – the biggest word of all – LOOK.
Everything you need to know is in there somewhere. The Golden Rule and love and basic sanitation. Ecology and politics and equality and sane living.
Take any one of those items and extrapolate it into sophisticated adult terms and apply it to your family life or your work or government or your world and it holds true and clear and firm. Think what a better world it would be if we all – the whole world – had cookies and milk at about 3 o'clock in the afternoon and then lay down with our blankies for a nap. Or if all governments had as a basic policy to always put things back where they found them and to clean up their own mess.
And it is still true, no matter how old you are, when you go out in the world, it is best to hold hands and stick together.
[Source: "ALL I REALLY NEED TO KNOW I LEARNED IN KINDERGARTEN" by Robert Fulghum. See his web site at http://www.robertfulghum.com/ ]
>Muckle, thanks for your answers..Lisa, glad you appreciated my points. Disgruntled microbiologist, your family history does sound infectious. Jamie, thanks for trying to answer even though personally I still don't understand your decision making process as you are on so many drugs and supplements. Dr. Snyderman, i think life is too precious not to ask if Dr. Brenner treats CLL; you already relapsed once….I truly hope you take my suggestion in the spirit it was meant.
Personally, my journey has been deeply influenced by Erik and Lisa even if I disagree on some things. It has been life altering and has not involved drugs and perhaps someday I'll be able to help others by writing more about it. I'm still learning.
Jill
>@RRM. "ALL five labs agreed that ALL 15 controls were negative"
Doesn't say that in the paper. Only says all for 3, and later when discussing one set of controls it says unnanimously agreed . Nothing about pedigreed negatives, or all agreeing on all samples.
You are also forgetting that the tests were not theirs, as no Trizol or other preservative was used and patients were on drugs known to produce false negatives.
Time to get over your conspiracy theory and face facts the study is a major embarrassment.
>Nope, it says that WPI, Lo, Ruscetti, Switzer and Coffin tested WB and plasma from ALL of those 12 donors and ALL of these labs agreed they were ALL negative.
As I have explained, the odds of then finding 9 out of these 12 to be positive, as well as finding 2 out of 3 lab controls (that were tested by all labs beforehand) as positive, are basically so low that they do not warrant serious thought.
And yes, I agree, this study has been a major, major embarrassment.
>Sorry, my post was directed at:
Anonymous September 25, 2011 6:22 PM
>I am talking about the study that received world publicity and was published recently in the NEJM. Only 3 patients I believe were treated and indeed the goal was to kill ALL B-cells. I read the actual paper as closely as I could and not just a review of it. You may be referencing a different study. However, if as you state, you only kill 1% of leukemia cells, that would not really show any change in the count and wouldn't be considered a reponse. In my study, my count which was going up, was reduced 30-40% and I hope will be reduced further this time. Before I was aware of the possibility of a retroviral influence I read the literature. The association of CLL with EBV was very inconsistant and was seen to any extent in only a couple of older papers, and then only about 25% of patients with CLL had associated EBV. Most papers were negative. I had my plasma checked for EBV DNA and that was negative and sent my leukemia cells to Mayo Clinic and their testing for the presence of EBV was negative. In the 1970s papers almost all of the patients with lymphoid malignancy had detectable MLRV in their tumor cells but not their normal cells.
The problem with training T-cells to attack a tumor is that in general there is no really tumor-specific antigen and that these T-cells can attack normal tissues which has happened. The only relatively tumor specific antigen is PSA in prostate cancer and there is a therapy that is available utilizing that called Provenge which adds on the average only 4 months of survival and costs about $150,000 for this 4 months. For the majority of cancer patients I believe this type of immunotherapy will not be valuable.
In my case, my treatment may be a form of corrective immunotherapy because if you look at my graphs it appears that the clonal gamma delta T-cells are exacerbating my leukemia and response of my leukemia comes as the clonal gamma delta T-cells decrease. These T-cells I believe have integrated retrovirus and viral proteins such as RT somehow causes expression of cytokine genes and proliferation genes (proto-oncogenes). The cytokines are partially responsible for the misery in CFS and also drive a concurrent malignancy which is called paracrine activity. In Peterson's original 300 patients, the 13 that developed defined lymphoma all had clonal gamma delta T-cells. He sent blood work out to LabCorp for this. I have screened so far 45 of my patients with various cancers, not just lymphoma and almost 50% have detectable clonal gamma delta T-cells. I use a Quest assay. This has never been looked for before in cancer in general but I owe the idea to do this to Peterson's original work.
In summary, I don't think immunotherapy of cancer will be very helpful but I think corrective immunotherapy-trying to reduce the numbers of clonal gamma delta T-cells will be. What the corrective therapy will be has to be determined. It may be ARVs as in my case but immunomodulating drugs such as lenalidomide may be valuable.
We believe that many patients with CFS have this clonal gamma delta T-cell proliferation but the test is not 100% sensitive and some who test negative will be positive on a later testing. I believe that treatment for CFS will eventually include targeting the clonal gamma delta T-cells. To make things more complicated there are probably other clonal expansions in CFS related to the virus for example B-cells (in my case leukemic B-cells) and perhaps even microglial cells which are derived from blood monocytes.
Michael Snyderman, MD
>I am testing ME/CFS patients with the Quest assays for TCR gene rearrangement. I already have a hit on the Leumeta, from a very small sample size. And it's quantitative!
Jamie
>Thanks for the concern. In my 40 years as a medical oncologist and hematologist I have treated hundreds of CLL patients and am aware of all the options and have a reasonably good ability to evaluate the newest popular treatment. Treatment has never before been shown to extend survival. Responses occur for sure but are temporary and bought with toxicity that is not acceptable to me.
I am happy with my decision to use ARVs. I believe we are learning important lessons as I have easily followed parameters and Judy did do my cytokines originally and showed that they dropped with my initial response. We will have more data associated with my recent response. Adding one RTI (tenofovir) to another RTI (AZT) that had worked but no longer was effective teaches us that RT is an important protein in my diseases. I am not done with my study. When I relapse again I will substitute fosamprenavir for the raltegravir. This PI has been shown to inhibit "XMRV" protease. What makes me excited about using it is that it prevents biological activation of Gag and Env which may also have a role. When and if I relapse after that, I will try low dose lenalidomide and learn more lessons.
Michael Snyderman, MD
>Gerwyn: "name another scientific hypothesis that explains the symptom spectrum of ME."
Epigenetic errors (hypomethylation) +
Environmental insults (either in utero, or gradually, throughout one's life, or both)
which weaken immune function and defenses against oxidative stress
which then deplete glutathione, SOD, catalase, etc..
A threshold is reached where antioxidant protection collapses, causing CFS, autism, ASD-spectrum illness, parkinson's, etc..
My point is that everyone is too focused on viruses and bacteria, even retroviruses (which according to the original science paper were found in more healthy people than those with CFS).
There are other pieces to this puzzle.
>@Gerwyn
Anyone can throw out spurious fiction as though it were facts to spin their own preconceived notions.
There was virtually no chance of WPI positives retesting positives because for some reason the patients were taking meds that would invoke false positives!
Show me the actual data:
Once the initial viremic phase is over, gammaretroviruses leave the blood and are thereafter only found in tissues and the antibody response disappears.
Show me the actual data/proof research article
The gammaretroviruses are only found in blood intermittently and are usually found as RNA when the virions enter the blood from other compartments.
Show me the actual data/proof research article
Using PCR and serology assays optimised to detect a synthetic clone, which does not exist in nature, is never going to be able to detect a HGRV if present.
Show me the actual data/proof research article
You dont have XMRV in your blood, you have a HGRV or possibly HGRVs.
Show me the actual data/proof research article
The WPI used VP35. They hypothesised that if the virus was present it would be at a low level. Firstly because gammaretroviruses behave this way in relation to blood and tissue and secondly perhaps this was why other had failed to detect such a virus previously. They also used many of the specifics of Silverman RT-PCR assay, including use of VP35.
Show me the actual data/proof research article
Although such retroviruses reside in tissue, virus does sneak out into the blood on occasion. To detect this highly specific conditions are required. PCR cannot begin to find low level virus in the blood without first lowering the annealing temperature and using RT-PCR. The right adjustments will pick up the virus. Again, pubmed has a wealth of papers on similar gammaretroviruses.
Show me the actual data/proof research article
This is on top of people being on meds that would have probably led to false negative results any way and forgetting to send all the negatives to all the labs for negative validation
Show me the actual data/proof research article
Thus far a family of gammaretroviruses have been detected in patients with ME
thus the hypothesis that grvs cause ME is a plausible parsimonious consilient hypothesis
Show me the actual data/proof research article
I think another point worth mentioning is that grvs infect and integrate into CD20 B cells
Show me the actual data/proof research article
destroying such cells gives some relief of symptoms but once the use of the monoclonal antibody stops the symptoms return. This would be expected if a grv infected progenitor cells in the marrow and homeostatic mechanisms engage to restore the CD20 B cell population
Show me the actual data/proof research article
After the initial period HGRVs are cleated from the blood and become indetectable by PCR
Show me the actual data/proof research article
Your 'scientific proof' are mere speculations that have no basis in fact and no other hypothesis.
Mikovits and the WPI stated the can detect hgrv.
Show the data and proof. They couldn't even find xmrv using their own techniques in a blinded study using their assays which now Mikovits stated their is no valid assays to detect xmrv.
The sequences that WPI and Mikovits uploaded to GenBank are the same sequences as VP62 and xmrv. Where are all the variations that indicate a new hgrv?
Finally, patients who claim this or that using this or that medical protocol procedure are all anecdotal at best. This is why some respond to some method of treatment while others do not. Without the identification of biomarkers with this disease, one must take into consideration that some of these patients may not have this illness, the disease could be in a early or latent stage, it could be a subset, etc. All information should be considered anecdotal at this stage.
>Jamie
I am not even going to attempt to follow what's been written in the comments here in any detail as my ME-addled brain is just not up to the task (I'm not referring to my intelligence here of course… :))
I'd just like to say, keep sharing your treatment experience. You are providing a valuable public service by doing so. My brain is crippled but my intelligence is intact so I am not unduly influenced or harmed by any of your posts – it's the overall journey that interests me, not the number of times you go on or off certain drugs or the reasons why. I think it's going to be the overview over time that provides the answers to their effectiveness, not the nitty gritty day to day details.
I thank all the people who are pioneering ARVs amid all the criticism and piousness. In my opinion, 50 people taking them over a couple of years will give us some idea of what the benefits and pitfalls of them are, and that info will start to filter through in a meaningful way eventually regardless of whether or not it is a formally conducted clinical trial. Though of course we always have the uncertainty of not knowing whether all 50 have the same illness, which will continue to be a confounding factor. Unfortunately, this critical and fundamental knowledge seems to be beyond the scope of health agencies to provide. Their lack of competency in this regard makes me not want to pay too much attention to anything they have to say with regard to the use of ARVs, I don't know about you.
I do not know what is going on with the XMRV validation/replication studies, it is far from clear. What I do know is that my conviction that this disease is caused by a retrovirus is unchanged regardless. It starts with an infection which is followed by dis-regulation of the immune system, and the infection appears to be for life. It has the hallmarks of a retrovirus and retroviruses have been glimpsed several times over the decades by serious researchers. My own illness began with a fever which is typical of initial HIV infection and I have symptoms such as altered body fat distribution, which is a feature of HIV. I look and feel like an AIDS patient. It seems a no-brainer to me.
I also know that the WPI are working hard to find out what is causing my illness. They are a group of dedicated, caring individuals who are making a difference in the lives of very sick people. There is no hidden agenda there, that is who they are, and they plough on in the face of unwarranted (in my book) attack. They have taken on a historically career-destroying and controversial illness and they appear to be sticking with it come what may. My eye (and money) continues to be on them. Hats off to them.
>Why do doctors/researchers not listen to the patients? So many have said, I was healthy, athletic, successful and happy. Then boom, I got this flu-like illness and I never recovered.
What besides a retrovirus can set someone up for a lifetime of of illness that continues to decline? The immune system cannot recover without treatment against the retrovirus.
We were not sickly, lazy, deconditioned, depressed losers looking for a way out of work and responsibility. So stop fooling around with our lives and do the right and honest research it takes to find good treatment.
It can happen to you or your loved ones also. Then you will change your outlook on this infection. The problem is that you will have no treatment because you have chosen to not listen to the patients.
Ann
>@Anon September 25, 2011 9:22 PM
Pubmed
For what they did in Lombardi, look in Lombardi.
For what they did in the BWG, look in Simmons.
For what a gamma retrovirus does, use pub med.
Not that hard now is it.