
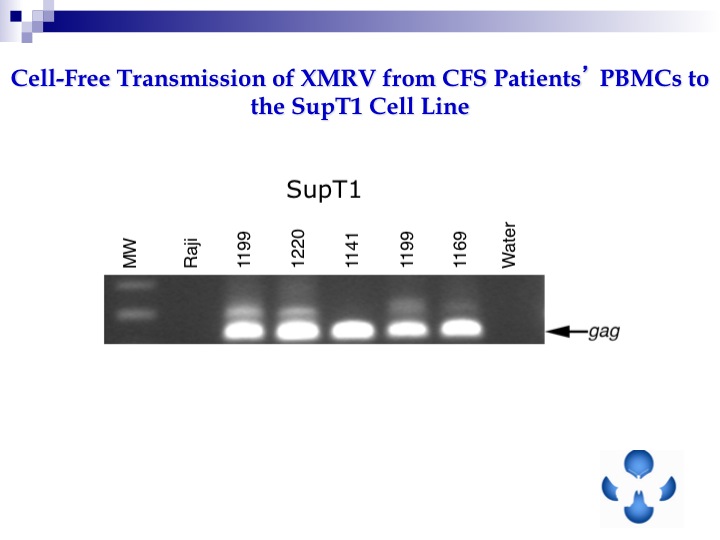
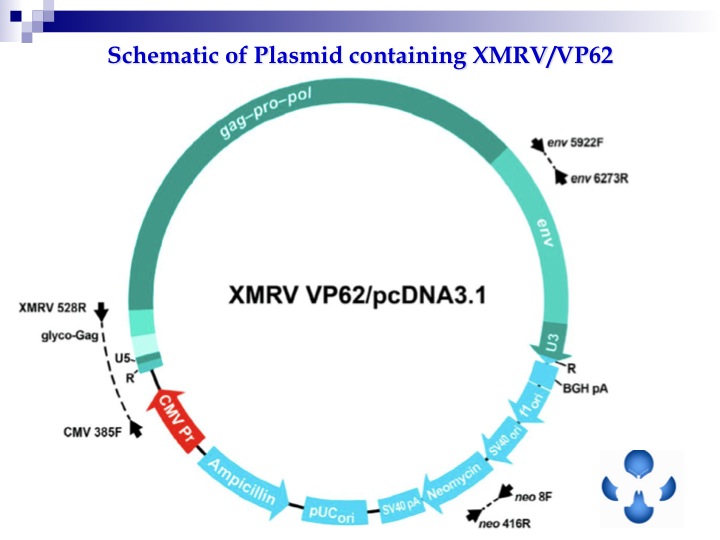
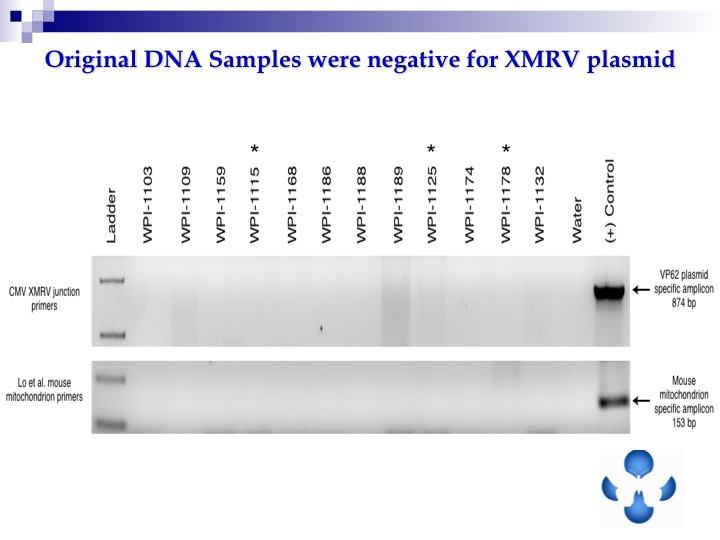
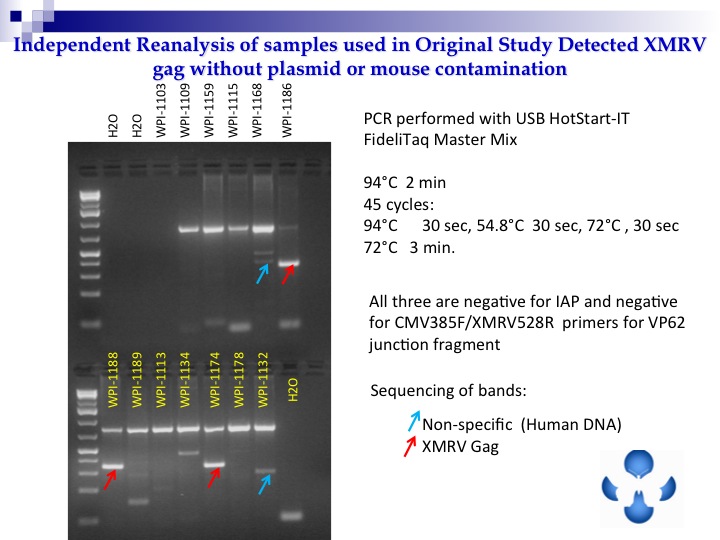
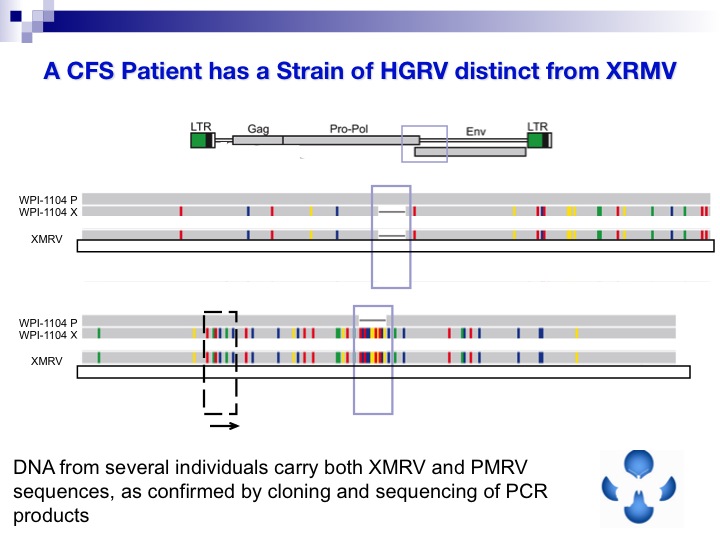
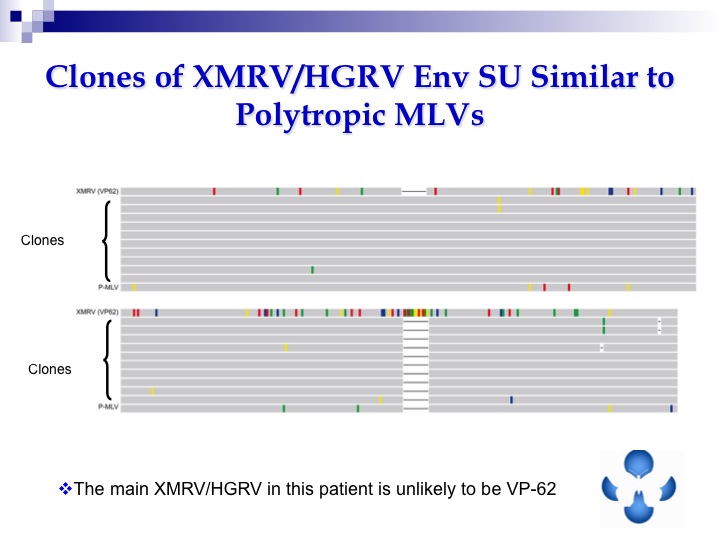
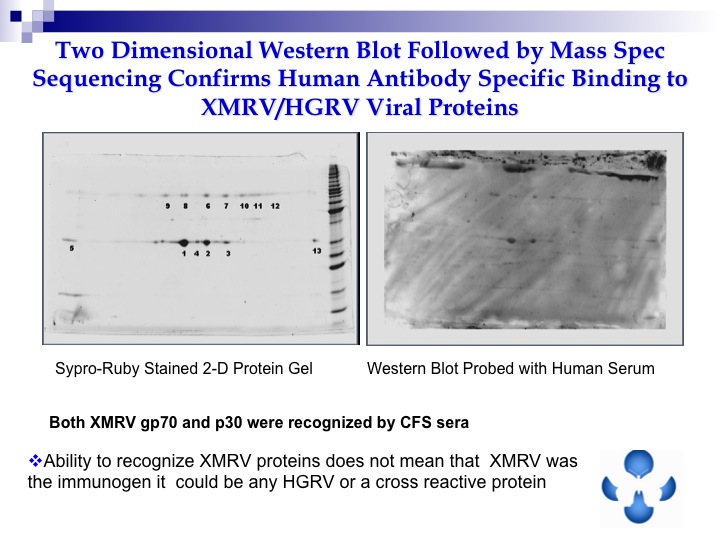
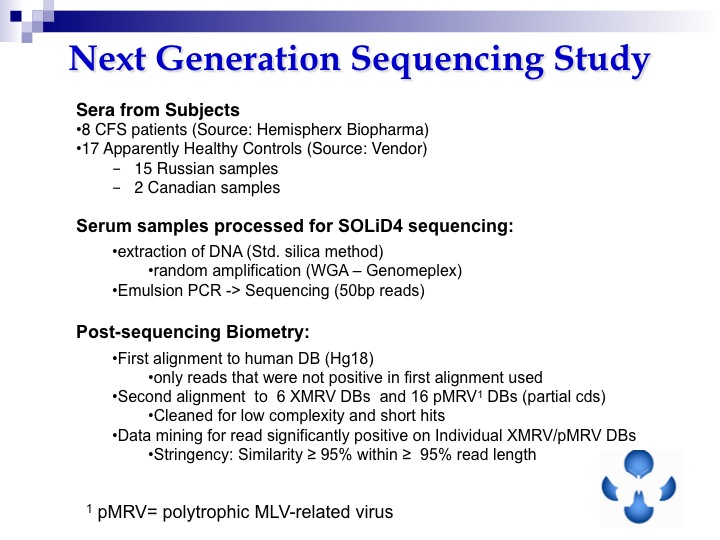
The intrepid Dr. Mikovits went up against Darth Vader today in Ottawa. In the face of incredible adversity, she took the heat. For us. And she points the way to the next step. Next Generation Sequencing. Here are her slides. Click each to enlarge. May the force be with her. Brava!






















>@RRM
Nope.
Now read again, where is the PBMCs and serology? Where are the other 4 labs? Come on you can figure it out.
Not all controls were screened by all labs. They were never shown to be negative before the study started.
>To Lisa Simpson:
"It starts with an infection which is followed by dis-regulation of the immune system…"
Reverse that, and I think you may be correct. If it indeed started with an infection, then many, many more people would be sick.
Say hi to Homer! (Seriously, best regards, hope your health improves!)
To Anonymous at 1:44AM:
Don't you mean, for what they THINK a gamma retrovirus does…?
No one knows what it does in humans.
Not that hard now is it?
>@Ann: "What besides a retrovirus can set someone up for a lifetime of of illness that continues to decline? "
How about petrochemicals, as in the case of Thomas Hennessy Jr., one of the most famous 'survivors' of a severe case of ME/CFS?
Or how about mercury poisoning, as in the case of Ric Carlson, the man who started ProHealth/ImmuneSupport.com?
Or how about stachybosis/mold, as in the case of the notorious Erik Johnson?
It's not always a virus.
>@Anon September 26, 2011 1:50 AM
No because I said gamma retrovirus, not human gamma retrovirus.
There is much we know about these types of retroviruses in general pulled from a wide range of hosts.
Not that hard now is it.
>@Anon September 26, 2011 1:56 AM
Nothing you have mentioned has any evidence associated with them to suggest they can cause what is ME. There is also no proposal of what to test to prove they could be the cause. Therefore they do not meet the minimum requirement to be called a hypothesis.
>I think it's time to change the title to "May the farce be with you". Move on, stop wasting time on this virus and look for a proper cause of CFS
>Why? We have 3 studies who are finding HGRVs. XMRV was the wrong name.
The Blood group messed up and made a study that was always going to produce mixed results like this.
So now we move forward. Studies will start again, because they all previously looked for VP62, that doesn't even exist.
>@Anon 2:39 AM
Who says XMRV was the wrong name.
Unless WPI and Mikovits keep moving the goal posts
which is it XMRV or HGRV
According to Mikovits and the WPI Lets see:
For 1 1/2 years Mikovits stated vehmently that ME/CFS patients have xmrv as proven through her pcr techniques. That xmrv causes a whole host of other diseases such Lymme, ms, lupus, Fibromyalgia etc.
On the negative papers she stated that they could not conduct proper PCR assays.XMRV is not a contaminate
Mikovits continued to strike a defiant tone, insisting that XMRV had not been ruled out as a potential cause of CFS.
"Anyone who says this is a lab contaminant has drawn the wrong conclusion and has done a disservice to the public," she told the journal.
She vowed to continue working to prove that XMRV is a genuine virus and is present in CFS patients. "The virus is real," she told Science. "I have isolated it from patients. I know it's there."
"The conclusion of the Blood Working Group was that we don't have a reproducible assay to detect XMRVs in the blood — not that they weren't in the patients at all."
She vowed to continue working to prove that XMRV is a genuine virus and is present in CFS patients. "The virus is real," she told Science. "I have isolated it from patients. I know it's an outbreak of XMRV.
These statements by Mikovits were quoted by various media outlets and journals.
But wait a second. In another journal she disavows xmrv. Where did that come from?
Dr. Mikovits said she stood by the theory that there was a retrovirus associated with chronic-fatigue syndrome, though not necessarily XMRV. "We have to dig in to find the right viruses. We need to keep looking," she said.
So which is it xmrv or hgrv? You can't have it both ways….well maybe you can with Mikovits. Apparently, she is confused on what she is finding in her lab if anything.
>Silverman confirmed it as the wrong name. He made a mistake and sequenced the VP62 that was in his lab. Now his part of the paper is retracted they have found the same virus as Lo et al. and Hanson. Which is very exciting as we now have 3 positive papers.
It also makes all studies using VP62 irrelevant as they were looking for the wrong virus. Essentially we are back in 2009 and the paper has only now been published.
>I think it's hard for anyone to deny that people in the modern world are exposed to a lot more chemicals than humans used to be.
I'm not talking necessarily about chemicals made by biotoxins here (though toxic mold is possibly the one that people routinely get the most exposure to). As it turns out (and this was a shock to me), even Erik's not just talking about biotoxins:
http://cfsuntied.com/blog2/2011/09/21/the-bleed/
The question is whether these chemicals have the potential of doing anything bad to us (and especially to subsegments of the population that are worse at detoxifying than others).
The amount of chemical exposure we get has been such a monumental shift in the conditions under which people live that I think it would be surprising if it had no effect at all. But of course, "scientists" usually discard the idea that anything could be bad for us until it's proven.
So the question is, what bad things might the accumulated crap we have in our bodies (as a result of more exposures and finite detox abilities) be causing?
I'm going to float a hypothesis. I don't know if it's true. It's just a hypothesis.
"There are lots of human gamma retroviruses floating around in the population, and there have been for thousands of years. Innately, they don't cause people any harm, because they rarely go active and come back under control fast if they do. However, insofar as people's bodies are filled up with a lot of crap, whichever ones are present — which is different for different people — go active and stay active, causing a range of related diseases that can be roughly categorized as CFS."
Is this consistent with what we are seeing in our search for HGRV's? In what ways does or doesn't it fit the facts?
Thanks much for your comments.
Best, Lisa
>@Anonymous September 26, 2011 1:48 AM
I HAVE figured it out my, but thanks again from the friendly advise.
The unescapable fact is that the 15 control samples were ALL pedigreed for serology and culturing by Mikovist/Ruscetti.
After that, Mikovits/Ruscetti designated 11 (or even 12) of these same 15 samples as positive by serology/culture.
Now, you seriously want to "discredit" this finding by arguing that some other labs did not do a PCR test, or that WPI did not pedigree PMBC from twelve controls?
Like I have explained, it doesn't matter: Mikovits/Ruscetti designated 11 (or 12) of those 15 patients as positive by culture/serology after they had pedigreed them as negative for culture/serology.
This is what makes these results extremely convincing. No amount of PBMC pedigreeing by WPI or any other lab can change that.
@Muckle
Hanson reportedly announced at her latest public talk that her PCR findings of "Lo-like" viruses were also due to contamination. She has found some sort of antibody response though, but it is unclear to exactly what pathogen, if any.
>@ Michael Synderman MD
Are you aware of this report and your take on it?
http://www.npr.org/blogs/health/2011/08/11/139536661/gene-therapy-breakthrough-trains-immune-system-to-fight-leukemia?ps=sh_sthdl
….Two reports out this week describe positive results using a gene therapy approach to treating a form of leukemia — chronic lymphocytic leukemia.
Although the study, explained in one report in the New England Journal of Medicine and another in Science Translational Medicine, was small — with only three patients in total — researchers have reason to be enthusiastic…
>If there is another scientific hypothesis re the cause of ME I would like to hear it
as for the BWG pmbcs not preserved in trizol means that pmbcs degraded so results meaningless
retroviruses cause neuroimmune diseasea particularily gammaretroviruses
around 40% of HIV positive people develop neuroimmune diseases
we now know that the viruses in the lombardi cohort were not VP-62
this is the only scientific hypothesis in town
>@Gerwyn
Here is a very plausible hypothesis for ME, published earlier this year by Lenny Jason.
http://www.scirp2.org/journal/PaperInformation.aspx?paperID=4275&publishStatus=2
If not using trizol caused degradation and the virus to die, how come WPI & Ruscetti repeatedly came up with positive results, including in over half of the negative controls?
Many things can cause disease of the nervous and immune systems. In ME the cause remains unidentified.
We now know that the viruses in the blood samples of the Lombardi cohort were exactly VP-62. It was contamination.
This scientific hypothesis just got run out of town.
Thank you and goodnight.
>Ed look at the slides above. It was not VP62.
>Dr. Snyderman,
Sounds like you have a plan…one you like.
Here is Dr. Brenner's page description (for anybody interested in this approach or knowing someone who might be):
Dr. Brenner's primary research interest is the use of gene transfer to augment the immune response to human tumors. In neuroblastoma, a recently completed study showed significant immunologic and anti-tumor effects from autologous tumor cells transduced ex vivo to express the interleukin-2 (IL-2) gene.
Based on additional animal models, this clinical study has been modified to include the genes for both lymphotactin (a T-cell chemokine) and IL2. This combination increases the anti-neuroblastoma immune response still further and it is hoped that we will see additional clinical benefits. We have also used phage display and differential display techniques to isolate T- and B-cell receptors with neuroblastoma specificity from the immunized patients.
Having cloned the relevant receptors, we are using gene transfer technology to generate hybrid T-cells with antitumor specificity. Similar studies are in progress for patients with leukemia and lymphoma, this time combining IL-2 with CD40L, a powerful co-stimulator molecule that in animal models appears particularly effective in CD40 positive leukemia and lymphomas.
Finally, in collaboration with Dr. Rooney's laboratory, we are continuing our studies using gene modified cytotoxic T lymphocytes to prevent and treat the Epstein Barr virus associated malignancies, immunoblastic lymphoma, Hodgkin disease, and nasopharyngeal cancer (NPC). By transducing dendritic cells with EBV antigens, we are able to generate potent immune responses against the weak EBV latency antigens expressed in Hodgkin disease and NPC. Studies in patients with EBV-positive Hodgkin patients have shown promising in vivo activity of CTL directed to these antigens with patients entering complete remission. The potential to increase the effectiveness of the T-cells in vivo using monoclonal antibodies directed to regulatory T-cells is now being evaluated in clinical trials.
—
From my understanding, the EBV is essentially *used* in some of these cancers, to retrain the immune system. My recollection of the case I mentioned, was that adenovirus (a common virus to which we have a marked immune response) was used ex vivo to train the t-cells. IE that virus makes the immune system really "mad". Put adenovirus in with the weak EBV antigens, and the immune system will be quickly trained to kill off any cell with either one.
It's a matter of training.
This approach is not big pharma…it is often individualized.
It's marvelous because it simply allows the immune system to do what it usually does so marvelously well.
You will see that in leukemia's they are using CD40.
There is a lot more info with a google search.
I don't recollect what was used in the lung cancer or pancreatic cancer patients I spoke with. This was a while ago. And I certainly didn't know about the recent study with 3 patients where all B cells were targeted.
—
I'm on a slow internet connection here in a place with wonderful blue skies and a few white puffy clouds so will leave it at that.
Jill
>Anonymous 2:56am.
Sorry, but you're wrong. You need to do more homework. But you probably won't, because you (and Gerwyn, rolls eyes) are blindly committed to the so-called hypothesis that has failed.
Like someone else posted above, I'd like to know who else besides Dr. Snyderman has improved dramatically using ARVs.
And Dr. Snyderman, I'm wondering what your opinion is of "Sue" on the PR boards, who has been trying a variety of ARV's for the last 18 months, with almost no improvement at all. And several emails from Mikovits.
>So good to see WPI forging ahead with intelligent research!!
>This go round when Mikowits retested the formerly positive patients did she use NEW blood samples from the same patients or was everyone retesting the same stored blood samples?
>@Anon 4:46 PM
Have you read the slides above?
What are you blindly committed to and not getting? It should be obvious that if you have a hypothesis you should be committed to it. It is a hypothesis not a religion, but that is how you test it. Could do with some other scientists now trying the same considering they have been looking for VP62 that doesn't exist.
As these viruses have almost no mutation rate, like HTLV, ARVs may only be affective in a fraction of patients as they are developed for viruses that use reverse transcriptase to propagate and not mitosis. Other more targeted treatments will need to be found.
>@Paula Carnes
It doesn't matter if the blood was stored or fresh. The patients were on medications that would produce false negatives, not all controls were screened by all labs, no preservative was used on PMBCs which would stop the WPIs assays from working and not all collection tubes were screened for contamination.
>@Paula Carnes
Everyone was testing freshly collected samples for this study.
@Ed
Gerwyn is only referring to the PBMC's. WPI/Ruscetti mostly detected positives using culture and serology assays.
Of course, Gerwyn's argument still doesn't make much sense, as the spiked PBMC's controls turned up positive for WPI 4 out of 5 times, as well as 5 out of 5 times for the six other labs.
This wouldn't have occured if the PBMC's had degraded because of bad storage practices, which indicates that the integrity of the PBMC's is not in question.
@Anonymous September 27, 2011 12:01 AM
WPI selected those patients. In fact, WPI could only come up with 10 positive controls. Think about this: both Singh and Levy had recruited more "WPI reported positives" for retesting in their respective studies.
The WPI could have asked anyone from some of the forums who was tested as XMRV+ and I am sure most would have been happy to do so.
This indicates that WPI were highly selective about who was about to enter this study. There is no doubt in my mind that WPI/Rusectti retested a lot of patients outside the scope of this study (as they had every right to, I might add, I know I would have with so much on the line), before selecting these patients as positives for this study. Which is why they preferred these 10 patients, some who had been on medication, over the tens/hundreds of patients (that weren't on medication) they could have easily recruited instead.
Bottom line: WPI did not just randomly enroll 10 of their previous positives from 1-3 years ago, knowing some of them were on medications that could affect results, AND not check up on this.
And yes, all negative controls were extensively screened by Mikovits/Ruscetti/Lo. All of them agreed all controls were negative before blinded testing, before they found them to be positive using the very same assays. I have already showed that even with sloppy screening, the odds of accidentally choosing 11 out of 15 "positive" controls are astronomically low under even the most optimistic conditions.
This basically shows that this finding of "11 out of 15 positive controls", is the result of false positivity. There is no credible alternative hypothesis that can explain finding 11 out of 15 negative controls to be positive.
>The controls were not all screened by all labs. Read the paper. So I don't know who you imagine checked them.
What do you think culturing involves RRM? I will give you a chance first.
"This wouldn't have occured if the PBMC's had degraded because of bad storage practices, which indicates that the integrity of the PBMC's is not in question."
What are you trying to imply here? There was no preservative used, you cannot rewrite that.
Singh only had two known positives and Levy would not have had access to information on who was positive. Neither replicated or diagnostically validated and in fact used a clone not found in nature. It is a red herring to claim anything else. In fact Lo et al. repeated their finding. What about that don't you understand?
What makes you think anyone was highly selective? Are you saying the controls were positives?
As all the patients in the study were on medications known to produce false negatives, why do you imagine this study was special and what magical assay do you believe would get around that?
Provide the quote that says all labs screened the controls. The paper doesn't say that. Again, what are you finding hard to understand?
>@ Anonymous September 27, 2011 1:10 AM
I can repeat this again and again, but I have never stated that all labs checked all negative controls. I am saying that ALL "positive labs" (Mikovits/Lo/Ruscetti) as well as SOME OF THE "negative labs" checked all of the negative controls. All of these labs unanimously agreed that these samples were negative.
You say: "Singh only had two known positives and Levy would not have had access to information on who was positive."
Singh had 14 "known positives". Only 2 of them were from the Lombardi et al. study, while the other 12 were positive through VipDx. As the WPI weren't restricted to selecting their positives from the Lombardi study either, the fact that they recruited less patients for this study than the number they supplied Singh with, clearly demonstrates that Mikovits was highly selective for this study.
As for Levy, your "point" actually strengthens my argument: even when Levy did not have access to who was positive, he still managed to enroll more positives. Therefore, the WPI should have had not problem recruiting more than 10 patients IF THEY WANTED TO DO THIS either. Again, this indicates that WPI were highly selective about who was about the enter this study. They didn't just "pick" 10 positives at random, hoping for the best.
you say: "What are you tring to imply [regarding the controls]"
I am not implying. You do realize that this is what spiked controls are for (i.a.): to validate the integrity of the sample. As all labs were able to detect the spiked XMRV in the PBMC samples, that shows there was nothing wrong with the preservation of the PBMC's.
You say: "What makes you think anyone was highly selective? Are you saying the controls were positives?"
No, I am talking about the "known positives". Given the fact that WPI only recruited 10 positives for this study, despite the fact they basically have the contact information of anyone who ever tested positive through their studies AND through the VipDX lab (which is probaly well over a 1000 in total), indicates that they were highly selective and only recruited positives that were validated multiple times, at multiple time points. In other words, these were positives that they were confident in reproducing.
You say: "Provide the quote that says all labs screened the controls. The paper doesn't say that. Again, what are you finding hard to understand?"
Please provide the quote in which I say that all labs screened the controls. Fact of the matter is that I didn't.
This is what I have stated:
ALL positive labs (Mikovits/Ruscetti/Lo) as well as SOME OF THE negative labs (Coffin/Switzer) tested ALL patients.
Sorry for being redundant, but there seems to be some confusion regarding this issue. I hope I have made my position clear now.
You say: "As all the patients in the study were on medications known to produce false negatives"
No, none of them were on medication that were "known" to lower the level of the virus to undetectable level. Not "all" of the patients were on the kind of medication you refer to either: the paper merely states that "several" were.
But again, Mikovits was responsible for slecting these patients. These results were clearly very important, not only for the millions of sick patients around the world, but also for the scientists themselves. Are you accusing the WPI of completely choosing the wrong patients for this study, when so much was at stake?
>It wouldn't matter if god selected the patients, if you are not able to then use the tests proven to work. No preservative, patients on drugs, not all controls screened and not all tubes checked for contamination.
>Dr. Snyderman,
I had a chance to go look for the study I think you are referencing, and if it's this one, it has nothing to do with Malcolm Brenner's work. It's not his study:
N Engl J Med. 2011 Aug 25;365(8):725-33. Epub 2011 Aug 10.
Chimeric antigen receptor-modified T cells in chronic lymphoid leukemia.
Porter DL, Levine BL, Kalos M, Bagg A, June CH.
Source
Abramson Cancer Center, and Department of Medicine, Perelman School of Medicine, University of Pennsylvania, Philadelphia, USA. david.porter@uphs.upenn.edu
Abstract
We designed a lentiviral vector expressing a chimeric antigen receptor with specificity for the B-cell antigen CD19, coupled with CD137 (a costimulatory receptor in T cells [4-1BB]) and CD3-zeta (a signal-transduction component of the T-cell antigen receptor) signaling domains. A low dose (approximately 1.5×10(5) cells per kilogram of body weight) of autologous chimeric antigen receptor-modified T cells reinfused into a patient with refractory chronic lymphocytic leukemia (CLL) expanded to a level that was more than 1000 times as high as the initial engraftment level in vivo, with delayed development of the tumor lysis syndrome and with complete remission. Apart from the tumor lysis syndrome, the only other grade 3/4 toxic effect related to chimeric antigen receptor T cells was lymphopenia. Engineered cells persisted at high levels for 6 months in the blood and bone marrow and continued to express the chimeric antigen receptor. A specific immune response was detected in the bone marrow, accompanied by loss of normal B cells and leukemia cells that express CD19. Remission was ongoing 10 months after treatment. Hypogammaglobulinemia was an expected chronic toxic effect.
Is this the study you were referencing?
If so, I don't think it's fair to dismiss one scientist's work by referencing a completely different scientist's work. But maybe I am wrong and there is another NEJM study?
In addition, "complete remission" does extend life. I'm not sure why you say these therapies, when they do put people into complete remission, don't extend life.
I also was curious about the mention of Peterson having inspired your look at the clonal T-cells. He has abandoned the retroviral hypothesis, so if he is still studying this himself, he must have another idea as to the cause?
Of course, you can't speak for Dr. Peterson. I'm just thinking out loud.
It's not that your immunomodulatory experiment, whether it is suppressing a retrovirus that contributes to your leukemia, isn't really interesting. It is. But I would like people reading this to be aware of work like Brenner's, since lives could be saved or extended–it is free, the clinical trial, if you are eligible, of course, and have failed chemo (or responded then failed).
Thanks.
Jill Neimark
>Thanks Justin for your comment. I needed a chuckle!
>Laurie, by the end of 2020, IT will be accepted that people with ME/cfs are infected with human gammaretroviruses. Chuckle.
>What are you chuckling at, please?
>Never mind, missed the context.(Probably.)
Anonymouses, could you please use a name or a handle?
>RRM said…
@Paula Carnes
Everyone was testing freshly collected samples for this study.
@Ed
Gerwyn is only referring to the PBMC's. WPI/Ruscetti mostly detected positives using culture and serology assays.
Of course, Gerwyn's argument still doesn't make much sense, as the spiked PBMC's controls turned up positive for WPI 4 out of 5 times, as well as 5 out of 5 times for the six other labs.
This wouldn't have occured if the PBMC's had degraded because of bad storage practices, which indicates that the integrity of the PBMC's is not in question.
In real life gammaretroviruses are integrated into B cells and mostly latent and in tissues
A spiked PMBC sample is not a match for in vivo conditions. Being able to detect a synthetic clone in a spiked sample means absolutely nothing and makes no statement at all about the integrity of the PMBC,s.The fact is that without trizol PMBcs would be degraded and any technique involving their culture or their activation would almost certainly fail
>Anon@12:52 aka Mystic Meg
So you're confident of HGRVs in ME/CFS, but not confident in anyone proving it for 9 years? Tell us what else you see in your crystal ball? Does Judy Mikovits win the Nobel prize for science and the WPI win the cleanest, contamination free lab award?
>@Ed
It will definitely be accepted by the world in ten years. Very comfortable prediction. Easy to see it is happening now. Took more than 10 years for HIV, which was wrongly called HTLV-III.
>@Muckle
Like I already explained: if the virus or the samples itself was degraded, you would not expect the controls to react normally. And they did.
I don't understand why you are posting that quote from Lombardi et al., as it doesn't seem to contradict anything I've said. By the way (and rather ironic): that quote is not about the DETECTION of XMRV, but about the detection of PROTEINS.
>@RRM
It is very difficult for you to understand this if you still refuse to read the entire paper. The controls were not all screened by all the labs. No one but the WPI and NCI/Ruscetti had validated assays, as Lo's staff used the incorrect assay and Lo does not have a diagnostically validated serology assay. Ruscetti performed no PCR, and the WPI were stopped from redoing the culture, their most sensitive assay.
Now you are aware that PBMCs were not treated with Trizol or an equivalent preservative and that no healthy controls were used with the PBMCs assays. What you are clearly still unaware of, as you have not read the paper, is that the lab controls were also at one time in the same lab as 22Rv1. So they cannot be assumed to be negative. And not all tubes were screened to assess whether they were virus free.
The NCI and WPI were also the only ones who could have validated the Lo samples, but they were never given those samples before the start of the blinding process. So they were not validated negative before the start.
Assays able to detect a clone, that does not exist in the wild, are not validated to detect integrated virus. No one but the WPI and NCI had validated assays.
>RRM can you name the proteins that are in gammaretroviruses?
>@Muckle
"The controls were not all screened by all the labs."
I have already addressed this but I'll just say it again:
– All three lab controls were screened by all labs
– All 12 blood donor controls were screened by all of the "positive" labs (Mikovits/Ruscetti/Lo) and two of the "negative" labs (Coffin/Switzer)
This means the controls were very well pedigreed, and the fact that the "positive" labs could not discriminate between pedigreed positive and pedigreed negative samples in blinded testing, is very convincing evidence that the "positive" labs' inititial papers were wrong.
"the lab controls were also at one time in the same lab as 22Rv1"
It is actually pretty ironic how you mention possible contamination with 22Rv1 during testing for the BWG. Do you realize that BY FAR the most positives were "detected" through Mikovits' and Ruscetti's serology tests? How could contamination with 22Rv1 account for that?
On a side note, the negative controls were not at any one time in the same lab (at least not before they entered the WPI lab, I must add). The paper explecitly addresses that "the cultivation of 22Rv1 cells, spiking of plasma, WB and PBMC and aliquoting of samples was all performed in a SEPERATE FACILITY than where the handling of clinical materials was done". The 'aliquoting' mentioned in the above quote refers to the aliquoting of the spiked controls BTW, not to the aliquoting of the negative samples. Perhaps you have misinterpreted this?
"..so [the Lo samples] were not validated negative before the start."
How would they have to be "validated negative"? They were validated positives through the Lo lab. Moreover, since Lo sent his 2010 samples to the Science paper investigators earlier, and those Science paper authors had reported that they had isolated XMRV (and that is bona fide XMRV) in blood samples from these patients, as well as an antibody response, the "Lo 2010 patients" actually were the best pedigreed from the lot.
"No one but the WPI and NCI had validated assays."
If the WPI and NCI had validated assays, they sure have invalidated them now. Judy Mikovits has stated that the conclusion of the BWG is that:
"..we don’t have a reproducible assay to detect XMRVs in the blood"
Furthermore, Mikovits has announced that they have suspended XMRV/HGRV testing through their commercial lab (VipDx/Unevx).
>RRM go and read about the negative controls and the controls. The controls were never tested with validated assays.
>"Furthermore, Mikovits has announced that they have suspended XMRV/HGRV testing through their commercial lab (VipDx/Unevx)."
Have a source for that? There is a rumour about XMRV going around, but that isn't the name for the viruses.
>@Anonymous September 28, 2011 3:38 AM
I don't have a source for Mikovits actual statement other than the one you are already referring to, but someone did in fact mail UNEVX and they confirmed. Source:
http://www.mecfsforums.com/index.php/topic,9652.msg114137.html#msg114137
>@RRM
Please read the paper and stop glancing over the paper. The samples were not screened by all the labs. Perhaps I can nudge you in the right direction. What methods were used to screen what controls? But before you go and find that information, if you are able, you must consider that there is no mention of any pedigreed controls in the study. You shouldn't get it wrong now.
"It is actually pretty ironic how you mention possible contamination with 22Rv1 during testing for the BWG. Do you realize that BY FAR the most positives were "detected" through Mikovits' and Ruscetti's serology tests? How could contamination with 22Rv1 account for that?"
There was no 22Rv1 in those labs. Now this one is easier than finding the assays used for screening each of the controls. Which lab was it?
"How would they have to be "validated negative"? They were validated positives through the Lo lab. Moreover, since Lo sent his 2010 samples to the Science paper investigators earlier, and those Science paper authors had reported that they had isolated XMRV (and that is bona fide XMRV) in blood samples from these patients, as well as an antibody response, the "Lo 2010 patients" actually were the best pedigreed from the lot."
Are you suggesting that it is never possible to validate a sample negative due to low viremia and preference for tissue? Lo's team changed to the unvalidated assay, so no one did pre-screen them. There is no source for stating those Lo patients are infected with XMRV, or that Lombardi investigators retested them. Lo did find the same HGRVs as the Lombardi authors, minus Silvermans mistake.
"If the WPI and NCI had validated assays, they sure have invalidated them now. Judy Mikovits has stated that the conclusion of the BWG is that:"
There is also no gold standard blood assay for other gamma retroviruses in other species, as they are rarely detected in blood due to low viremia, preference for tissue and CpG islands.
>RRM, where does your source, still not an official announcement, mention XMRV? That's not the name. It is HGRV.
>@Muckle
"Perhaps I can nudge you in the right direction."
"Now this one is easier than finding the assays used for screening each of the controls. Which lab was it?"
Resorting to comments like these is not very useful.
If you have evidence that one of my assertions is wrong, please provide said evidence. Saying that "it's in the paper" does not help.
"There is no source for stating those Lo patients are infected with XMRV, or that Lombardi investigators retested them."
Unlike you, I will back up my assertions with evidence:
http://www.youtube.com/watch?v=n3kdU5FhH2U
It's at 14:45 in the video. Judy Mikovits explicitly states that Frank Ruscetti isolated XMRV from Lo's revisited cohort and that Rachel Bagni showed an immune response in those same patients.
Now that I have shown you conclusive evidence that Lo's 2010 patients were "pedigreed" positive for HGRV's by Ruscetti's lab, will you adapt your opinion accordingly?
@Anonymous September 28, 2011 4:10 AM
My source explicitly states both XMRV and HGRV:
"When I asked whether they are accepting new HGRV/XMRV test requests, they said, "No, not at this moment."
I agree it's not an official announcement, and I didn't assert there was. I think the source confirms my interpretation of Mikovits' statement at the conference.
>@Muckle
My initial reply was caught by (I suppose) the spam filter. I hope it will be viewable later. In the meanwhile, my most important point is the fact that the Lo samples WERE VALIDATED by the Lombardi investigators.
Since I guess the spam filter filtered my post because of the link, to check for yourself, please do the following.
– Go to youtube
– Search for "Mikovits Sweden"
– Select part 2/4 of the Mikovits talk of 02/12/2010 (second link)
– Go to 14:45 in the video
– You will find that Mikovist herself confirms that both (Frank) Ruscetti (virus isolation) and Bagni (immune response) pedigreed the Lo 2010 patients as being positive using their own methodology.
>@RRM
The paper is not difficult to read. The Lo samples were never validated by the WPI or NCI. Do you know the difference between what occurs in a study and what occurs in separate work?
>@Muckle
I asserted the following:
"since Lo sent his 2010 samples to the Science paper investigators earlier, and those Science paper authors had reported that they had isolated XMRV"
You replied:
"There is no source for stating those Lo patients are infected with XMRV, or that Lombardi investigators retested them."
Do you concede the fact that this statement from you was flat-out wrong and, if so, how does that change your view of the situation? If it doesn't matter, why did you make such an arguing point of it?
Regarding your other questions: I agree the paper is not difficult to read and I do know the difference between what occurs in a study and what occurs in seperate work.
However, since the Simmons study explicitly states that labs were free to use assays "of their own choosing", Ruscetti was free to use the assay that he found the XMRV/HGRV in the Lo samples with.
You can spin this all you like, but the bottom line is that Ruscetti should have been able to reliably detect the XMRV/HGRV in the Lo samples if it was there.
>@RRM
The Lo samples used in the BWG were not pre-screened by the WPI or NCI. Do you know the difference between what was a part of the Blood study and what was not? I can see you do not. Otherwise you be claiming that the CDCs retesting of WPI samples proves that there was no contamination present. And I am aware you are trying to avoid the scientific data on this research field.
The labs were not free to choose. If they had been, there would have been Trizol used with the PBMCs and the WPI would have been allowed to finish their culture panel.
>@Muckle
Your analogy is invalid. Contamination enters a sample at a given moment, for instance during a 42-day culturing process. The contamination does not exist in the patient – otherwise it wouldn't be contamination for the purpose of this subject.
Therefore, checking samples that have not been through that 42 day culturing process, or samples that have not been through the WPI's lab at all, cannot be tested for contamination at WPI.
On the other side, if those Lo samples did contain XMRV in June/July 2010, as well as a detectable antibody response, it is to be expected that these experiments can be succesfully repeated a few months later. That is if, unlike contamination, the XMRV was really in those patients' blood to begin with.
The labs were free to choose. It's pretty ironic that you've accused me of not properly reading the Simmons paper, when it literately states:
"All nine laboratories used XMRV/P-MLV nucleic acid amplification testing (NAT), serological and/or culture assays of their own choosing"
Mikovits is the (co-)author of that statement. I am sure you know that storage protocol is not "part" of an assay, and not being able to report results because of contamination does not change the fact that she was free to choose to culture and she indeed cultured samples.
I am sure that, if Mikovits so requests and her cell line is again clean, the kind people at BSRI will gladly provide her with some duplicate samples.
>New blog by Prof. Vincent Racaniello
http://www.virology.ws/2011/09/27/trust-science-not-scientists/
"…pursuing the CFS-gammaretrovirus hypothesis is a disservice to those with CFS, and detracts from efforts to solve the disease. There are no data to support such an association, and to suggest that a lab contaminant, XMRV, has pointed the way to a bona fide etiologic agent seems implausible."
>@RRM
Silverman has said it was his error. I think the problem is your own now.
Now you are admitting that the WPI and NCI didn't screen the Lo samples. Finally! You really shouldn't get involved in discussion such as these when you struggle to follow the text.
No too soon, you are trying again.
The Lo samples were not screened by the WPI or NCI and not all assays were used on the controls and negative controls. You are selectively cherry picking out sections of text that when in context prove you to be wrong.
Mikovits did not write the Blood working group paper. Really where did you get that idea from.
You really are the silliest person. Blood samples are not a cell line and there is no way of knowing if mycoplasma contaminated those before they arrived at the WPI. They have been prevented from completing this section of the study by the BWG.