
One morning an elderly man was walking on a nearly deserted beach after a big storm had washed up thousands and thousands of starfish. He came upon a boy who was picking them up and throwing them back into the ocean, as eagerly as he could.
Puzzled, the older man looked at the young boy and asked, “Little boy, what are you doing?”
The youth responded without looking up, “I’m trying to save these starfish, sir.”
The old man chuckled aloud, and queried, “Son, there are thousands of starfish and only one of you. What difference can you make?”
Holding a starfish in his hand, the boy turned to the man and, gently tossing it into the water, said, “It will make a difference to that one!”
It is all well and good to say that now that XMRV is dead, science can get back to its orderly, stepwise process; they even get to say, we told you so. And I say what I have said all along: millions of patients need treatment now. It is not a static situation. It is a progressive disease, slow, but lots of people are circling the drain. Many new cases that might be easier to treat sooner rather than later… that might respond more completely to arv’s. New babies being born with it. Should we wait a decade to start to find out, in a systematic way, if existing treatments might not affect it? It is incumbent upon the medical and pharmaceutical industries to think about the disease in concept and find solutions, not sit there doing nothing until Virus X is found; that approach already hasn’t worked for decades. It is quite likely that it won’t turn out to be a one virus, one disease, one treatment paradigm. If it were that simple, it would have been found already. So I find myself sitting with real patients, in the here and now, framing the illness as I have outlined here over the last year and a half. I still find the model we are evolving useful in a clinical context.
In my last practice, my interest was peak performance with respect to brain function, no matter the degree of injury or illness. I worked with the things that I found useful, personally and for my patients, most of whom had already exhausted their medical options. I was undiagnosed at that time. I knew I was sick, but it wasn’t too bad, and I knew that conventional medicine had nothing to offer me. It occurred to me now and then that I had some sort of less than MS. Other possibilities occurred as well. I tried to fit it into PTSD, but there were too many physical manifestations, hypertensive crises, arrhythmias, atypical migraines, malaise, this or that instability. I could exercise without problems for a decade. I used to say that whenever something went wrong with my body, it was undiagnosable. And I was CFIDS aware. That state of not knowing made me well suited to being a doctor of last resort. My armamentarium then was HBOT, neurofeedback, nootropics (cognitive enhancers), nutraceuticals, herbs and bioidentical hormones. I found discontinuing unnecessary drugs to be a powerful treatment modality. And I tried to create the space for the less tangible, but no less powerful healing that can happen in the context of connection and relationship.
So far, I am using pretty much the same gentle, yet powerful modalities that I used before, when I didn’t know what I was doing:), and I’m having some beginner’s luck. I am turning to these treatments first, because I know from experience, they work, and now I have a framework that gives me a better idea why. Pulsed, high dose normobaric oxygen is the most powerful and easy to deliver treatment that I have to offer. My patients so far are pretty uniformly impressed. Nobody that has rented a concentrator for a month has returned it, unless to buy one. Responses range from a little helpful to “wow”. There is a short term effect and a long-term additive effect, as I observed with HBOT in practice. It seems one of the craziest things in all this that such a simple thing has been denied us. I wonder about why, and can’t come up with much. It will never be studied, because it can’t be patented. It might accelerate aging, but the longevity folks think it’s the opposite. It needs to be more carefully dosed for patients with seizures and a few other things. Mostly, it’s probably because doctors don’t understand the gas laws, and so are uncomfortable with it. They can handle it when it comes out of a wall in a hospital, where it’s use is sanctioned, and there’s a respiratory therapist to hook things up. Otherwise, if you have COPD or are dying, you can have it. Sometimes insurance will cover it for cluster headaches, or migraines, common in our patient group. I am prescribing oxygen, for an hour a day and prn, at 10L/min by non-rebreather mask (has a reservoir and check valves), or 5-6L/min by simple mask for patients who bought lower flow concentrators (two are improving with this).
Here are a couple of references that address the oxygen paradox: Why might high dose oxygen be good for us, even though we have increased oxidative stress at baseline?
Oxidative stress, antioxidant defenses, and damage removal, repair, and replacement systems. Davies: Cells, tissues, organs, and organisms utilize multiple layers of antioxidant defenses and damage removal, and replacement or repair systems in order to cope with the remaining stress and damage that oxygen engenders. The enzymes comprising many of these protective systems are inducible under conditions of oxidative stress adaptation, in which the expression of over 40 mammalian genes is upregulated.
HIV: reactive oxygen species, enveloped viruses and hyperbaric oxygen. Baugh: ROIs repeatedly have been shown to be virucidal against enveloped-viruses, like the human immunodeficiency virus (HIV). Hyperbaric oxygen therapy (HBOT) increases the production of ROIs throughout the body, leaving no safe harbor for the virus to hide outside the genome. This technique already has been tried on acquired immune deficiency syndrome (AIDS) patients, with exciting results.
As I am finishing my first six months of practice, Ali is coming into her own, with great courage. She has enrolled for an online undergraduate program at U Mass, and will start next month. She has been dating, but still mostly staying home rather than venturing out. Right now, she is deep in the process of confronting that she is probably physically able to do more things away from home, but confined by habit and the limitations of the past. It is hugely more difficult for her than for me to emerge, without a former life to go back to.
Ali credits oxygen and modified Meyer’s cocktail infusions with her slow but continued improvement. She tells me when she feels the need for an infusion. We are still tinkering with the best formula for her. She uses oxygen 4-5 times a week, according to her own instincts. She has come to use it prophylactically for PEM, when she knows she’s overdone it. It is impossible to know what role antiretrovirals are playing in maintaining her gradual improvement which began with the cessation of Lyme treatment and was also obviously impacted by Deplin and treatment for PCOS (polycystic ovarian syndrome). Our concentrator has been broken for a couple of weeks and when the replacement came, she grabbed the mask, exclaiming “Oxygen! Mana of the Gods.” For me too, oxygen is the most tangible thing I have. It impacts my sleep directly.
 |
| click to enlarge |
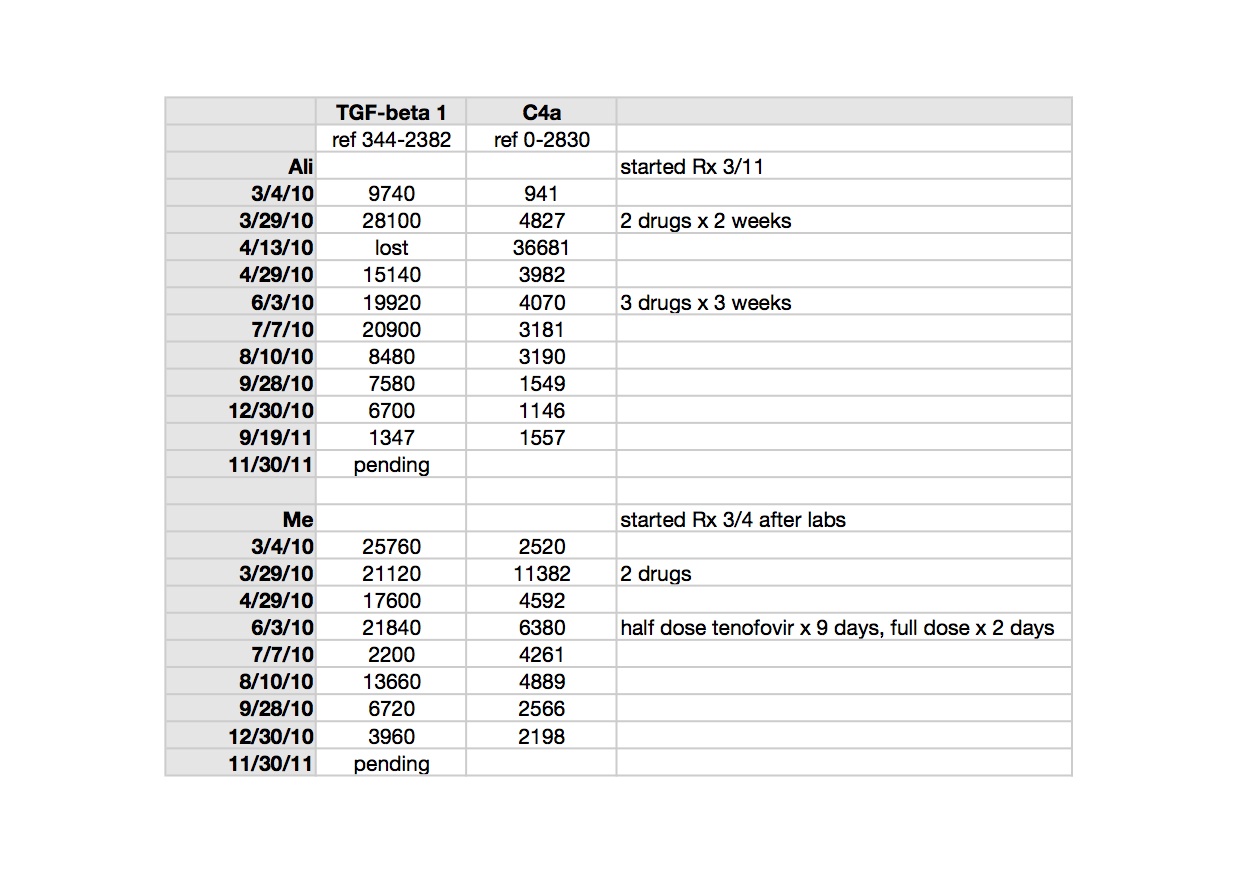
TGF beta-1 is a peptide involved in many cellular functions, including the control of cell growth, proliferation, differentiation and apoptosis. Here is a recent paper suggesting TGF beta-1 as a marker for CFS: Up-regulation of TGF-β1 mRNA expression in peripheral blood mononuclear cells of patients with chronic fatigue syndrome. Zhang. It is tempting to speculate that TGF beta-1 could be involved in the clonal expansion we are starting to think about with respect to the pathogenesis of ME/CFS and related leukemias; not forgetting that simple animal retroviruses replicate mitotically, by clonal expansion.
TGF beta-1 is implicated in the pathogenesis of Marfan’s Syndrome, which my husband’s uncle, husband and son have; in our family it appears to be more obviously expressed in each successive generation. Elevated TGF beta-1 is implicated in the pathophysiology of Marfan’s. My husband and I both had different, subclinical manifestations of illness when we met, but most, though not all, of his were attributable to Marfan’s. Marfan’s is an autosomal dominant genetic condition where chromosome 15 encodes for a defective protein which is necessary to bind TGF beta-1 to keep it sequestered to normal levels (oversimplified model). Losartan, an ARB (angiotensin receptor blocker) has been shown in clinical trials of Marfan’s patients to lower TGF beta-1 and slow the onset of the most serious consequence of the disease, aortic root dilatation. My biological father had a body habitus consistent with Marfan’s and I may be an Ehlers Danlos variant, becoming more flexible with age and exacerbations of illness. I have minor features of both conditions. Both Marfan’s and Ehlers Danlos seem to be over-expressed in the ME/CFS patient group, already showing up in my tiny practice. Here is an excellent article which considers related disorders with respect to abnormal TGF beta-1 signaling: Transforming growth factor-beta signaling in thoracic aortic aneurysm development: a paradox in pathogenesis. Jones/Ikonomidis.
>Dr. jamie – i want to thank you for sharing your experiences and treatment protocols, and to tell you now before i quit joining in the discussions on this blog. I find much of what you talk about to be helpful and well -reasoned, but the same cannot be said about the discussions held between your supporters and detractors. Some of you may consider gossip and speculation about the doctors and researchers to be stimulating discourse but i find it tedious in the extreme, and find it detracts from the discussion as a whole. I know not many share this feeling, which is why i'll only be a passive partaker in the future. Again, thanks for doing what you do and i'll keep checking in from time to time to sample the blogging you should be proud of.
>It is somehow comforting to me to be talking again about the everyday, practical approaches to treatment of people with M.E. This is where I, too, am now focused, although of course, my focus is on treating my own illness. I thank you, Dr. Jamie, for discussing these treatments. I find it very helpful to hear about your experience and Ali's experience.
>I'm watching my whole family circling the drain. My only hope is that the mistakes made through this whole ordeal will be recognised, and soon. Only then will there be hope for the next generations. I do not wish for my son and granddaughter to suffer this same fate. That is more than I could bare.
>Another excellent blog Dr. J. Keep 'em coming. Just don't stop.
https://www.youtube.com/watch?v=pafY6sZt0FE
peace out :o)
>Thanks very much for the info on oxygen :)
>Jamie, I have been doing oxygen (just using tanks and breathing for periods each day, but also HBOT several years ago) for over ten years now, and I have continued to have a progressive decline. I would say in my case oxygen is helpful, but I don't notice it stopping the disease progression when I start it after stopping for awhile. It simply sometimes makes me feel better, and is helpful for MCS exposures and to a lesser extent PEM recovery.
I am curious if at some point you have comments on how to get oxygen covered by insurance. Many ME/CFS patients I know seem to have the problem Dr. Cheney noted on one video of having normal pulseox readings but showing physical signs of hypoxia (because oxygen molecules are not decoupling from hemoglobin): needless to say this makes insurance coverage difficult.
I am also intrigued by the Marfan connection — I am fascinated by Marfan Syndrome and wondered if a more subclinical version could account for some of the cardiac problems in ME/CFS. Do you see a cardiac connection in any of your patients or does TGF beta-1 relate at all to cardiac function? I just looked up more on Marfan cardiac issues and found it interesting that Marfan Syndrome can cause subclinical diastolic issues: http://onlinelibrary.wiley.com/doi/10.1002/clc.4960250905/abstract
Thanks for more fascinating food for thought.
>"she is prevented from discussing the case by her attorneys."
This makes it impossible for Dr Mikovits to discuss the errors and faults made in the negative papers and blood working group. So why is the WPI proceeding with this?
XMRV is over as Mikovits would agree because the viruses they discovered were not "XMRV". The retraction of Silvermans full sequencing, Mikovits/Ruscetti having never got Silvermans assay to work, they new polytropic env regions in the genbank, all show the viruses they found are not "XMRV". We need Dr Mikovits back in a lab now, so again why are the WPI doing this if Annette claims to want to continue with the research? Lombardi does not have the experience and is not a PI.
>XMRV with prostate cancer isn't dead either. There is no evidence of any contamination in those positive papers and the methods used are not prone to contamination. It is VP62/XMRV that was never alive and is now dismissed from related to the ME MLV-related viruses claim, which is alive and well.
>It is nice to see the old X Rx back.
>As for me, I will keep picking up those starfish. Keep up the good work, Dr. D-J.
”Who saves one man saves the entire universe” says the Talmud.
I am one of those using the lower pressure oxygen. It seems to help me quite a bit – not a cure but I feel better when I use it every day.
>Cheers DrDJ
PCOS seems to be quite prevalent in our patient group, is this anything yr finding yrself DrDJ.
>Hi Dr Jamie,
Thank you for continuing to write. It is always informative.
I've recently been diagnosed with Hashimoto's thyroiditis (I am also diagnosed with ME according to the CCC since 2008) and am now taking thyroxine.
I'd be interested in knowing how common Hashimoto's is amongst people with ME and what treatment people receive for it. Can it be reversed?
Thank you!
Nicky Reiss
>Thank you for your informative post. It's always good to get back to possible treatments for this disease.
I agree with the impatience in the research and its complexities. Since I think my illness is getting worse, I would like treatments to be found quickly that help.
I once tried vit. C infusions and each time I could not get out of bed for 3 days, not to do anything. I was terribly weak. I had to stop it, and also it was very expensive. To pay that much and end up incapacitated was not a good thing.
I had to write something over the weekend and what I have to go through to do this is something that perhaps only other CFS sufferers know. I have to type every single thing — thought and fact down– and work from the writing as I can't retain several facts at once nor think unless it's written down.
Anyway, we'll stay tuned to the posts.
>Thanks for the info re oxygen, and thanks for showing your lab results. The labs speak to a retroviral causation, as arv's took down the disease markers. I'm saving for a concentrator. Even second hand, they cost!
This is a nit-pick for other readers, Jamie, not for you. You said "It is all well and good to say that now that XMRV is dead, science can get back to its orderly, stepwise process; they even get to say, we told you so"
But XMRV is not dead. See Dr Cheney's blog Changing status of XMRV / HGRV research
"The strongest supportive study to date was reported by Dr. David Strayer out of Hemispherex Inc, (Philadephia, PA) at IACFS/ME in Ottawa and showed that 7/8 CFS cases and 2/17 controls were positive for XMRV using Next Generation Sequencing (NGS) technology available at Roche Labs in Germany. NGS is not susceptible to mouse contamination and demonstrates that XMRV is in fact integrated into human DNA which means it is a human virus."
http://www.cheneyclinic.com/changing-status-of-xmrv-hgrv-research-2/843
>Jace, and others. Here in NZ we can hire oxygen machines with a doctors note. Just thought you may not have thought of that.
Jamie. My partner Al has ME severely. His family are very tall and gangly and skinny Does this go with Marfans?. He seems to have what I call 'extensions'. Both at the wrists and ankles. ie extra bits. His father has a had a triple A (only found serendipitiously when a med student was checking a kidney stone and found an aneurysm as well – geez he was lucky). Is this typical of Marfans? I'm now wondering whether he could have it, as well as ME. I must look it up on wiki. Thanks once again for sharing your knowledge
>WOW ! cheers Jace,
that's huge news about HGRVs,
what will happen now, any ideas anyone?
>FISH, IHC, serology and EM are also not susceptible to contamination. Every time they try to knock it down they skip over this evidence.
>Thank you for sharing this information. Perhaps those in this discussion could be able to get this treatment and glad they will be helped. Good for the "starfish" who can bypass the basic fundamental problems with diagnosis. But the vast majority of the community with a CFS diagnosis would never come close. ME/CFS is not a diagnosis but will become the same trap, will obliterate ME, with no testing and treatment. Talking of ME will be a sham as it will become CFS.
>3 CHEERS FOR DR CHENEY!!!
WOOHOO!!
>"It is all well and good to say that now that XMRV is dead, science can get back to its orderly, stepwise process; they even get to say, we told you so."
Your subtle sarcasm against research is more than apparent. Post after post you continue to bash scientific research and researchers that are trying to help ME patients in the long run. If science proves that there a retrovirus does not cause ME than more power to them and I'm grateful they can come to an unbiased conclusion. This would allow more research to proceed to find whats truly causing this very complex disease.
Seriously, you need to stop attacking science in your blog. We are not your enemies, nor are we implicit in some grand conspiracy to silence research in a biased manner.
All we want is to cure this intractable disease, very much as you do.
>@ anon 10:31 am
I must have missed the "subtle sarcasm". I know Dr. D-J very well. She was saying that the science will go on, as science usually, but not always, does, in a carefully planned way. Meanwhile, as a clinical doctor, she will continue to treat patients based on her clinical experience with thousands of Lyme and CFS patients and based on other doctors' work with patients. She cannot sit back and say, "Oh, well, the scientific jury is out on retroviruses, so the patients will just have to wallow in their misery.
I would love to read of your credentials and your research experience with retroviruses since you are a scientist. What do you think of Dr. Cheney's brief summary of the evidence for a retrovirus?
>Anon 10:31 AM.
I didn't intend for it to be subtle. My family and most of the readers of this blog have been forsaken by both the medical and scientific communities for many years, some for decades. Now that a couple of scientists have decided that our plight is worthy of study, in the closet for now, until the patent issues are resolved, we are supposed to forget the decades of neglect and abuse, hold our collective breath?
I watched my amazing, brilliant daughter become housebound, while doctors acted like she was nuts or I was nuts. And now I'm supposed to thank the powers that be? If you are at a private institution, this isn't directed at you, but at those scientists who work for our government, who tucked it away so nobody had to pay to treat it, while millions more got sick. My daughter need never have gotten sick.
And I don't think cure is possible, at this time. But effective treatment may already exist on the shelves of every pharmacy. Nobody is looking. That is an outrage.
Jamie
>"Seriously, you need to stop attacking science in your blog. We are not your enemies, nor are we implicit in some grand conspiracy to silence research in a biased manner."
Not going to take your word on your claims of being a scientist. Why hide if you are claiming to support science?
You cannot no much of the history of the disease to say there has not been some sort of conspiracy. Have a look at who gets funding, what secret files on ME are held, the multiple attempts to reclassify the disease, use of inadequate MRI machines, attempts to alter the entry criteria for studies, the disgusting letter posted on the notice board of the CDC. If I gave this some thought I would soon mark your head spin. How about doctors trying to section the careers of sick dying patients? What you won't admit is that none of this is about science. Science doesn't come into it. Every paper that has failed to find the viruses failed to clinically validate their assays. That is not science. The fallen paper Paprotka et al. was the worst kind of politically motivated paper that had no foundations to stop research into these viruses. And who can forget that comment from a HIV campaigner at CROI. Why are you not condemning any of these actions?
>Also Anon 10:31 AM,
Both systems, "science" and "medicine", are completely broken and cannot be fixed in their current form. No fault of the individuals trapped therein. In general, I am more a believer in stupidity and negligence than conspiracy. Laziness, entropy and just plain being wrong are more likely the major contributors to the situation, but anyone who looked at the politics and history of the disease would wonder.
Jamie
>Oh I don't discount laziness, negligence and being wrong. But certain events have been recorded. We can read about the plans and how they were then achieved. That does constitute conspiracy. After all it is only two or more people working together for a shared goal. It is not the fault of those now stuck in this system, but they should consider if they have the courage to tear it down.
>Anon 10:31 AM,
We don't have an enemy list but we have only a few but fearful friends.
Scientists are supposed to be objective and completely open until the data is in. The data isn't in yet and we still get emails from people calling themselves scientists who want to bury the retroviral etiology of CFS. We see posts from the University of Pittsburgh saying that it is not safe to do research to prove there is a virus.
What type of science is this? This is intimidation and negativity!
My personal response to ARVs proves that there is a retrovirus and integration studies are in progress. We had hoped to do deep sequencing but because of the intimidation factor, the scientist has backed off. Instead of people who call themselves scientists showering us with scorn, we challenge them to help us with this.
Michael Snyderman, MD
>". We see posts from the University of Pittsburgh saying that it is not safe to do research to prove there is a virus. "
Wow! Makes me sick. They are ultimately putting their own lives at risk and their families and friends. Why are they scared to research this scientifically?
>Why isn't it safe, says the U. of Pittsburgh, to study a possible retroviral link to CFS? What do they mean?
I was very dismayed at some in the "scientific" community who were verbally abusive to Dr. Mikovits, whether she is right or not. The whole way that happened was stifling to researchers, I would think.
David Tuller's article on the history of the CDC's inaction, I thought was quite revealing.
I can recognize lack of concern, downright neglect, lack of scientific curiosity and accepting the path of least resistance on the part of researchers.
I don't accept those but I recognize that. What is hard to accept is that the CDC misappropriated funds for CFS research. How do they get away with that? There was no accountability.
I do know that there are federal cutbacks in medical research, and that it takes a lot of action and pressure to get diseases researched properly. It took a movement with HIV and AIDS.
I don't know what it will take with CFS. I wish we could sit in like Occupy is doing in D.C. But we don't have the energy to do it.
Even the CFSAC sessions looked incredibly controlled, with more time spent telling callers with CFS their time limits than actually listening or vowing to do something.
I surely can say that the government should be faulted for its inaction, negligence, and so on.
But maybe more research will happen as there are many researchers now.
>Well said Kathy. Misappropriation of funds would also be a conspiracy.
Having safety as an issue for scientists is getting into dark territory. But how can they risk not becoming infected?
>Why was HIV-negative AIDS swept under the rug?
http://www.aegis.com/pubs/gmhc/1992/GM060803.html
>There is a link at the CFIDS Assn. website to an article in ScienceInsider, which although slanted against Dr. Mikovits, does quote her attorney. He sounds good.
She has a court date in January.
>New docket activity in Mikovits case copied and pasted from:
http://www.ccwashoe.com/public/ck_public_qry_doct.cp_dktrpt_docket_report?case_id=CV11-03232&begin_date=&end_date=
Can anyone with legal background translate what is going on?
[copy and pasted below:]
01-DEC-2011
02:28 PM Mtn for Stay … Jones, Esq., Dennis Neil
Entry: DEFT'S EMERGENCY MOTION TO STAY CIVIL PROCEEDINGS PENDING OUTCOME OF CRIMINAL CASE – Transaction 2620403 – Approved By: ASMITH : 12-01-2011:15:51:57
02-DEC-2011
04:01 PM Motion … Jones, Esq., Dennis Neil
Entry: DEFENDANT'S MOTION FOR AN ORDER, EXTENDING THE TIME FOR MOVING PARTY TO FILE A RESPONSIVE PLEADING – Transaction 2623873 – Approved By: JYOST : 12-02-2011:16:53:25
02-DEC-2011
04:04 PM Motion … Jones, Esq., Dennis Neil
Entry: DEFENDANT'S MOTION FOR LEAVE TO FILE MOTION FOR RECONSIDERATION OF ORDERS RE PRELIMINARY INJUNCTION – Transaction 2623882 – Approved By: JYOST : 12-02-2011:16:44:10
02-DEC-2011
04:56 PM Declaration Jones, Esq., Dennis Neil
Entry: DECLARATION OF JUDY MIKOVITS RE: DELIVERY OF ITEMS PURSUANT TO ORDER GRANTING PRELIMINARY INJUNCTION – Transaction 2624186 – Approved By: MCHOLICO : 12-05-2011:10:58:49
02-DEC-2011
05:10 PM Declaration Jones, Esq., Dennis Neil
Entry: DECLATATION OF JUDY MIKOVITS – Transaction 2624230 – Approved By: MLAWRENC : 12-05-2011:08:09:48
05-DEC-2011
04:13 PM Notice … Hall, Esq., Ann Osborne
Entry: NOTICE OF INTENT TO TAKE DEFAULT – Transaction 2626738 – Approved By: ASMITH : 12-06-2011:07:46:28
07-DEC-2011
04:51 PM Mtn Ord to Show Cause Hall, Esq., Ann Osborne
Entry: MOTION FOR AN ORDER TO SHOW CAUSE REGARDING WHY MIKOVITS SHOULD NOT BE HELD IN CONTEMPT AND SANCTIONED FOR DISOBEYING COURT ORDERS – Transaction 2632996 – Approved By: LMATHEUS : 12-07-2011:16:58:07
07-DEC-2011
05:13 PM Ord Shortening Time
Entry: ON PLAINTIFFS' APPLICATION FOR AN ORDER TO SHOW CAUSE REGARDING WHY MIKOVITS SHOULD NOT BE HELD IN CONTEMPT AND SANCTIONS FOR DISOBEYING COURT ORDERS – Transaction 2633053 – Approved By: NOREVIEW : 12-07-2011:17:14:15
>The issue is who had legal access/ownership of any materials, who had the materials, who returned what to the police. As pertinent is how RRM and Billy, both who are hostile to Mikovits and the research were able to post raw Lombardi data when materials are claimed "stolen". It is also important to ask why Annette Whittemore would say Judy took her notebooks from the lab and yet the WPI claim they did not know who had them. This was also at a time when Max claims to have them. Ownership and access to scientific melaterials goes to the heart of progress. The world will be watching.
>@Anonymous 11:31 pm:
Wow! Your legal-beagle insight is so sharp and helpful. If only everyone were as unbiased and clear-sighted as you are. Thanks for clearing everything up for us!
>ME is the disease. CFS is a sociopolitical construct. There is no such illness as CFS. CFS is like saying X=ABCDE. Find the cause of X. We are promoting a faulty shifting construct, and wonder why people don't get it. ME/CFS is even worse as half truths are worse than lies. Without an accurate diagnosis with a specific agreed upon definition that is used consistently there still be no meaningful research results. This is why there has been no progress.
CDC has told the truth: "The name myalgic encephalomyelitis (ME) was coined in the 1950s to clarify well-documented outbreaks of disease; however, ME is accompanied by neurologic and muscular signs and has a case definition distinct from that of CFS." ME is not CFS. Yet we now have these groups conspiring to officially combine them as ME=CFS=ME/CFS. This is what Wessely does. Then they create these phony "ME" groups which are or combined with CFS. Other than the few lucky starfish, most will be doomed. We could do much better.
>Jill,
I appreciate your point, but I am in favor of more inclusive, not exclusive definitions. I think we have a good enough understanding of the disease to recognize early cases that don't manifest the full blown syndrome. Your definition of ME, would have missed me for almost a decade, and still misses my husband, who is definitely affected, in my clinical opinion. I think it is a mistake to throw all the patients who don't meet criteria for the worst form of the disease to the dogs. We are stronger if they are with us. Strength in numbers. Many of them will be where we are eventually.
Jamie
>Jamie, I appreciate your medical treatment info and it works for you (or those starfish who can get it) but not in the real world. The "CFS" defs can (?) include ME but gives inappropriate and harmful treatment recommendations so how does that 'help' us? According to your objections and under the current situation, the sickest ME patients are thrown to the dogs by the demeaning and trivializing CFS. How is this justification? Most ME patients do not agree and will not go along with the CFS ME/CFS crowd.
>@anon 7:46
Past history of the disease is important is it not? And why should the community view the researchers any differently then any other fallible section of society? Researchers are no different to anyone else. Do you deny the misappropriation of funding that occurred?
>Jill,
It is an artificial division, having nothing to do with the clinical reality. Quite a few of my patients are coming with relatives who are a little sick, spouse, parent, child. Should I think they have something different? The division is causing large subsets of patients to be treated incorrectly. The Lyme and CFS doc's still think they are treating different diseases, to the detriment of both groups of patients. Should you have to see 2 different doctors to consider both antivirals and antibiotics? Should AIDS patients with PCP see a different doctor than patients with some other opportunistic infection? I believe that CFS and autism are essentially the same disease; they are occurring in the same families, as our family survey will show (we will update everybody soon).
Seeing the tip of the iceberg as a separate disease might facilitate certain types of research, but hurts lots and lots of people, who are excluded, left in the dark. The most exclusive definition is designed to prove that it's a real disease, rather than address the clinical reality, that it is many related diseases. Even the "classic" patients who were healthy, went down with a viral illness and never got up again, turn out to have had preclinical illness earlier in their lives, if a careful history is taken.
It's like saying that you don't have cardiac disease until you have a massive MI, COPD until you are oxygen dependent, or cancer until it metastasizes. We are capable of doing better than what you are asking for, medically. It may even be possible to avoid the crash, if our eyes are wide open and we use everything at our disposal when it happens, not after 6 months, or years, of neglect.
Jamie
>That said, I'd be happy to drop CFS and call it all ME. I use "post-infectious encephalomyelitis" a lot. I still like non-HIV AIDS best.
Jamie
>Jill and @ Peggy also,
The treatments I write about "work", but they are palliative at best, and may require synergism to bring about and maintain functional improvement. I write about them here so that everyone can think about them, even if you are not one of my starfish. It is possible to find practitioners almost everywhere who would cooperate with the things I am suggesting. In some states, in this country, naturopaths can prescribe and be very helpful. Nurse practitioners and alternative doctors sometimes have an outlook that will allow for a good healing relationship.
Jamie
>Paula Carnes @December 7, 2011 10:45 AM asks…
"….What do you think of Dr. Cheney's brief summary of the evidence for a retrovirus?"
There is a comment by "Jason" (perhaps the same "Jason" that posted here on Xrx previously?) over on ERV's blog regarding the Cheney "public relations" post on NGS data. It's comment #42, posted on December 8, 2011 11:21 AM, in response to a similiar question. Makes the point that many of the new NGS technologies still incorporate a PCR amplification step, so the "flaws exposed in the current primary PCR technology" (e.g. contamination, mis-priming, PCR artifacts, etc.) are still germane. Pubmed shows no follow-on work by Dr. David Strayer of Hemispherex. Like Alter and Lo, still waiting to hear the next chapter.
>Jamie, Regarding treatment in general, sans labels or formal case definitions of any kind, I think you do just fine. I would come to you as a clinician (or Dr. Enlander, Cheney etc). You know what to look for and what to do (better than most). But we cannot base everything on this.
And it is easy to find drs who would do these things? Absolutely not. Not with CFS. Reality is, safe to say ALL CFS drs have it or are somehow directly involved, so your baseline is way off from what's in the general millieu.
Divisions are no more arbitrary than for anything else. So with CFS – is all CFS chronic Lyme? And I recognize the autism connection, but same dx? There may be overlap of many illnesses but there are still distinctions that warrant recognition. There are now "chronic illness" approaches which mainly focus on the role of inflammation. I agree that it is probably to a great degree but do we abandon all diagnoses? There has to be some way to identify relatively homogeneous groups and especially for research if we want real effective treatments (western medicine is reductionist until a new paradigm takes over that may be better ). But ME patients do not want to be dx with a fatigue syndrome.
>Jill, I hear you. And we agree, it is more than semantics. It is about right to treatment, which is why I don't think only the tip of the iceberg is worthy of consideration. We need to look at the whole elephant.
Jamie
>Jamie Deckoff-Jones MD said…
"That said, I'd be happy to drop CFS and call it all ME. I use "post-infectious encephalomyelitis" a lot. I still like non-HIV AIDS best."
Jamie, this is the issue. The "it." "CFS" is not an it but a heterogenous syndrome. Absent markers, illnesses are what they are defined to be. The defs of ME and CFS do not match up and thus are not the same. Calling "CFS" ME will not really help. ME can be called ME, or something else if the features are maintained and recognized.
>"Wow! Your legal-beagle insight is so sharp and helpful. If only everyone were as unbiased and clear-sighted as you are. Thanks for clearing everything up for us!"
How do any of us here know what has gone on? All we can do is ask questions.
>"many of the new NGS technologies still incorporate a PCR amplification step, so the "flaws exposed in the current primary PCR technology" (e.g. contamination, mis-priming, PCR artifacts, etc.) are still germane."
Those flaws do not apply to IHC, FISH, serology or EM of a budding maturing virion, but all have been used and found these human gamma retroviruses.
"Pubmed shows no follow-on work by Dr. David Strayer of Hemispherex. Like Alter and Lo, still waiting to hear the next chapter."
The study is ongoing. Does it not concern you that people are being told it is not "safe" to study these viruses?
>Anybody got a ref to the not safe thing?
>Jamie, Thanks and I think we basically do agree. The clinicians on the frontline should be helping as many "starfish" as possible. We should take on the advocacy issues.
>I think the name CFS demeans us. It doesn't say anything. The very word "fatigue" is a total misnomer. It's like comparing the proverbial molehill to a mountain. And it does demean us, where our so-called fatigue lays us flat for days, not able to go out and mail a letter or buy groceries or take a shower.
We're sick as dogs here with CFS. I know I had other illnesses before this one, which probably were just precursors of the CFS.
A lot of people with CFS are homebound, unable to work or take showers, get their own food, go up or down stairs, etc. They are very sick.
They should not be diminished.
The thing is the government isn't taking either CFS or ME seriously, and pursuing research aggressively for either one or both.
So we're all suffering and need action. We do need to stick together and make demands on research and treatment.