
One morning an elderly man was walking on a nearly deserted beach after a big storm had washed up thousands and thousands of starfish. He came upon a boy who was picking them up and throwing them back into the ocean, as eagerly as he could.
Puzzled, the older man looked at the young boy and asked, “Little boy, what are you doing?”
The youth responded without looking up, “I’m trying to save these starfish, sir.”
The old man chuckled aloud, and queried, “Son, there are thousands of starfish and only one of you. What difference can you make?”
Holding a starfish in his hand, the boy turned to the man and, gently tossing it into the water, said, “It will make a difference to that one!”
It is all well and good to say that now that XMRV is dead, science can get back to its orderly, stepwise process; they even get to say, we told you so. And I say what I have said all along: millions of patients need treatment now. It is not a static situation. It is a progressive disease, slow, but lots of people are circling the drain. Many new cases that might be easier to treat sooner rather than later… that might respond more completely to arv’s. New babies being born with it. Should we wait a decade to start to find out, in a systematic way, if existing treatments might not affect it? It is incumbent upon the medical and pharmaceutical industries to think about the disease in concept and find solutions, not sit there doing nothing until Virus X is found; that approach already hasn’t worked for decades. It is quite likely that it won’t turn out to be a one virus, one disease, one treatment paradigm. If it were that simple, it would have been found already. So I find myself sitting with real patients, in the here and now, framing the illness as I have outlined here over the last year and a half. I still find the model we are evolving useful in a clinical context.
In my last practice, my interest was peak performance with respect to brain function, no matter the degree of injury or illness. I worked with the things that I found useful, personally and for my patients, most of whom had already exhausted their medical options. I was undiagnosed at that time. I knew I was sick, but it wasn’t too bad, and I knew that conventional medicine had nothing to offer me. It occurred to me now and then that I had some sort of less than MS. Other possibilities occurred as well. I tried to fit it into PTSD, but there were too many physical manifestations, hypertensive crises, arrhythmias, atypical migraines, malaise, this or that instability. I could exercise without problems for a decade. I used to say that whenever something went wrong with my body, it was undiagnosable. And I was CFIDS aware. That state of not knowing made me well suited to being a doctor of last resort. My armamentarium then was HBOT, neurofeedback, nootropics (cognitive enhancers), nutraceuticals, herbs and bioidentical hormones. I found discontinuing unnecessary drugs to be a powerful treatment modality. And I tried to create the space for the less tangible, but no less powerful healing that can happen in the context of connection and relationship.
So far, I am using pretty much the same gentle, yet powerful modalities that I used before, when I didn’t know what I was doing:), and I’m having some beginner’s luck. I am turning to these treatments first, because I know from experience, they work, and now I have a framework that gives me a better idea why. Pulsed, high dose normobaric oxygen is the most powerful and easy to deliver treatment that I have to offer. My patients so far are pretty uniformly impressed. Nobody that has rented a concentrator for a month has returned it, unless to buy one. Responses range from a little helpful to “wow”. There is a short term effect and a long-term additive effect, as I observed with HBOT in practice. It seems one of the craziest things in all this that such a simple thing has been denied us. I wonder about why, and can’t come up with much. It will never be studied, because it can’t be patented. It might accelerate aging, but the longevity folks think it’s the opposite. It needs to be more carefully dosed for patients with seizures and a few other things. Mostly, it’s probably because doctors don’t understand the gas laws, and so are uncomfortable with it. They can handle it when it comes out of a wall in a hospital, where it’s use is sanctioned, and there’s a respiratory therapist to hook things up. Otherwise, if you have COPD or are dying, you can have it. Sometimes insurance will cover it for cluster headaches, or migraines, common in our patient group. I am prescribing oxygen, for an hour a day and prn, at 10L/min by non-rebreather mask (has a reservoir and check valves), or 5-6L/min by simple mask for patients who bought lower flow concentrators (two are improving with this).
Here are a couple of references that address the oxygen paradox: Why might high dose oxygen be good for us, even though we have increased oxidative stress at baseline?
Oxidative stress, antioxidant defenses, and damage removal, repair, and replacement systems. Davies: Cells, tissues, organs, and organisms utilize multiple layers of antioxidant defenses and damage removal, and replacement or repair systems in order to cope with the remaining stress and damage that oxygen engenders. The enzymes comprising many of these protective systems are inducible under conditions of oxidative stress adaptation, in which the expression of over 40 mammalian genes is upregulated.
HIV: reactive oxygen species, enveloped viruses and hyperbaric oxygen. Baugh: ROIs repeatedly have been shown to be virucidal against enveloped-viruses, like the human immunodeficiency virus (HIV). Hyperbaric oxygen therapy (HBOT) increases the production of ROIs throughout the body, leaving no safe harbor for the virus to hide outside the genome. This technique already has been tried on acquired immune deficiency syndrome (AIDS) patients, with exciting results.
As I am finishing my first six months of practice, Ali is coming into her own, with great courage. She has enrolled for an online undergraduate program at U Mass, and will start next month. She has been dating, but still mostly staying home rather than venturing out. Right now, she is deep in the process of confronting that she is probably physically able to do more things away from home, but confined by habit and the limitations of the past. It is hugely more difficult for her than for me to emerge, without a former life to go back to.
Ali credits oxygen and modified Meyer’s cocktail infusions with her slow but continued improvement. She tells me when she feels the need for an infusion. We are still tinkering with the best formula for her. She uses oxygen 4-5 times a week, according to her own instincts. She has come to use it prophylactically for PEM, when she knows she’s overdone it. It is impossible to know what role antiretrovirals are playing in maintaining her gradual improvement which began with the cessation of Lyme treatment and was also obviously impacted by Deplin and treatment for PCOS (polycystic ovarian syndrome). Our concentrator has been broken for a couple of weeks and when the replacement came, she grabbed the mask, exclaiming “Oxygen! Mana of the Gods.” For me too, oxygen is the most tangible thing I have. It impacts my sleep directly.
 |
| click to enlarge |
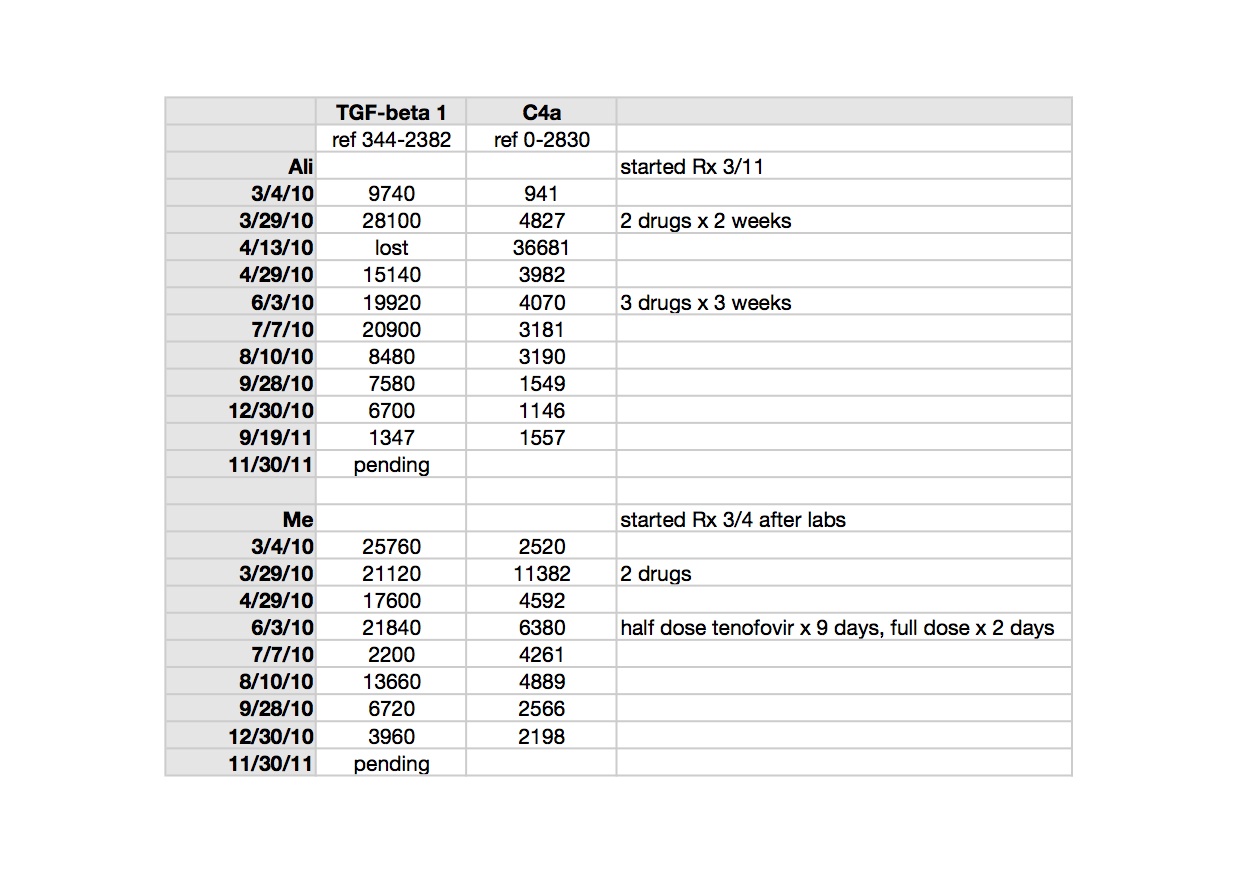
TGF beta-1 is a peptide involved in many cellular functions, including the control of cell growth, proliferation, differentiation and apoptosis. Here is a recent paper suggesting TGF beta-1 as a marker for CFS: Up-regulation of TGF-β1 mRNA expression in peripheral blood mononuclear cells of patients with chronic fatigue syndrome. Zhang. It is tempting to speculate that TGF beta-1 could be involved in the clonal expansion we are starting to think about with respect to the pathogenesis of ME/CFS and related leukemias; not forgetting that simple animal retroviruses replicate mitotically, by clonal expansion.
TGF beta-1 is implicated in the pathogenesis of Marfan’s Syndrome, which my husband’s uncle, husband and son have; in our family it appears to be more obviously expressed in each successive generation. Elevated TGF beta-1 is implicated in the pathophysiology of Marfan’s. My husband and I both had different, subclinical manifestations of illness when we met, but most, though not all, of his were attributable to Marfan’s. Marfan’s is an autosomal dominant genetic condition where chromosome 15 encodes for a defective protein which is necessary to bind TGF beta-1 to keep it sequestered to normal levels (oversimplified model). Losartan, an ARB (angiotensin receptor blocker) has been shown in clinical trials of Marfan’s patients to lower TGF beta-1 and slow the onset of the most serious consequence of the disease, aortic root dilatation. My biological father had a body habitus consistent with Marfan’s and I may be an Ehlers Danlos variant, becoming more flexible with age and exacerbations of illness. I have minor features of both conditions. Both Marfan’s and Ehlers Danlos seem to be over-expressed in the ME/CFS patient group, already showing up in my tiny practice. Here is an excellent article which considers related disorders with respect to abnormal TGF beta-1 signaling: Transforming growth factor-beta signaling in thoracic aortic aneurysm development: a paradox in pathogenesis. Jones/Ikonomidis.
>If we want to have move forward we need to attach objective measures to entry criteria.
>AnonymousNonRetrovirologist, would you agree with this?
"”There is increasing concern that in modern research, false findings may be the majority or even the vast majority of published research claims…Conflicts of interest are very common in biomedical research, and typically they are inadequately and sparsely reported…Prestigious investigators may suppress via the peer review process the appearance and dissemination of findings that refute their findings, thus condemning their field to perpetuate false dogma. Empirical evidence on expert opinion shows that it is extremely unreliable…Highly prejudiced stakeholders may even create a barrier that aborts efforts at obtaining and disseminating opposing results…”
Ioannidis JP. Why most published research findings are false. PLoS Med. 2005 Aug; 2(8): e124. http://medicine.plosjournals.org/perlserv/?request=get-pdf&file=10.1371_journal.pmed.0020124-L.pdf
— John P.A. Ioannidis, MD, Dept. of Hygiene and Epidemiology, University of Ioannina School of Medicine, Greece; Institute for Clinical Research and Health Policy Studies, Dept. of Medicine, Tufts-New England Medical Center, Boston
>To get at billions of dollars of research monies for CFS/ME, what first needs to occur is for people need to write to Congress and demand a "Re-Appraisal of AIDS." AIDS patients are simply more CFS patients. And it's already a well-accepted fact that HIV is not the cause of CFS/ME.
https://writerep.house.gov/writerep/welcome.shtml
http://www.senate.gov/general/contact_information/senators_cfm.cfm
In the fight for humanity.
http://www.cfsstraighttalk.blogspot.com
>Anonymous @December 8, 2011 2:19 PM stated:
"Those flaws do not apply to IHC, FISH, serology or EM of a budding maturing virion, but all have been used and found these human gamma retroviruses."
While obviously true in that PCR-specific pitfalls do not apply to these techniques, they all have their own unique flaws, weaknesses and Achilles Heels: antibodies can broadly cross-react and/or be selectively reactive (why will an antibody work fine in a Western, for example, yet fail when used in ELISAs?); and it looks like a little MLV can go a long way, witness 22RV1 cell line shedding replication-competent virions unbeknownst and undetected for years in many labs (with reports of contaminated lab robots and horizontal transmission between cell cultures in spite of bleach, UV and the usual precautions) ; and we have the still-never-quite-answered questions regarding the "non-germane" use of 5-AZA brought to light during the "Slidegate" incident as popularized on ERV's blog. And an EM can show nascent virus, fine, but in light of what has been revealed, can your EM image determine if the particle is an emergent infectious endogenized XMRV replicating within host, or an XMRV sourced from contamination (low sequence diversity, identical integration sites), or something else (ancient HERVs?) resurrected and brought forth by judicious use of a demethylating reagent? (Once one's credibility goes, it goes all the way, doesn't it?)
"The study is ongoing." Would be interesting to see more details on the work when (or if) published.
"Does it not concern you that people are being told it is not 'safe' to study these viruses?"
Sorry, must have missed that particular thread. "Safe" as in "personal safety"? Or "safe" as in "not jacking up your career"?
Back in the 1980's I spent the better part of two years all garbed up like "Andromeda Strain" in a BSL3+ facility working up blood and plasma from patients with what was then called "non-A/non-B hepatitis". Double-gloved, double-gowned, surgical facemasks, booties, no sharps, everything taken out had to be pass-thru autoclaved, tubs and pans and spray bottles of bleach everywhere, all surfaces bleached and UV irradiation before and after work, the whole nine yards. So precautions have to be taken, sure, when dealing with suspected virulent human pathogens. It looks like XMRV is handled quite adequately by our innate immune systems, so unless immunocompromised, XMRV is probably not a dire infectious threat (and even so, it's not detected in HIV patients, for example).
As for the career aspect: there are probably a lot of folks wishing they'd never heard of "XMRV". But people's memories are actually pretty short: witness Dr. Lo's career–no one really takes him to task over his earlier "mycoplasma–AIDS" and "mycoplasma–CFS" hypotheses. And note that University of Pittsburgh professor O'Keefe is not brandishing forth her BPH-related-viruses as the cause of autism, Gulf War syndrome, ALS, ME, or Parkinson's disease–is that not a "safe" career move, not overstating/overselling your data? Dr. Mikovits should have just moved on without the cloak-and-dagger intrigue now alleged in Max Pfost's affadavits. And as a general rule, it's probably not a "safe" career move to steal stuff, even stuff that may legitimately be yours, from your ex-employers, especially if your ex-employers are rich and powerful, very well-connected and very unhappy with you.
>Anonymous @December 8, 2011 5:28 PM said…
"AnonymousNonRetrovirologist, would you agree with this?
"”There is increasing concern that in modern research, false findings may be the majority or even the vast majority of published research claims…Conflicts of interest are very common in biomedical research, and typically they are inadequately and sparsely reported…Prestigious investigators may suppress via the peer review process the appearance and dissemination of findings that refute their findings, thus condemning their field to perpetuate false dogma. Empirical evidence on expert opinion shows that it is extremely unreliable…Highly prejudiced stakeholders may even create a barrier that aborts efforts at obtaining and disseminating opposing results…” [from: Ioannidis JP. Why most published research findings are false. PLoS Med. 2005 Aug; 2(8): e124]"
Echoes of Thomas Kuhn? Probably more of a basic psychological manifestation of our fundamentally selfish, dark and twisted human natures, don't you think? And couldn't this base theme be applied to any human endeavour? (Isn't the Old Guard always trying to put down the Young Turks regardless of field of activity?)
And, of course, the ironic thing is that, by having been published in the literature, isn't this very work now at risk of being itself a false finding?
>Hello NonRetrovirologist:
What did that germ turn out to be – the one you were working with in the 1980s? I am just curious.
Dr. Montagnier also thought that mycoplasma might be a necessary cofactor for HIV to progress to AIDS. It may well contribute in AIDS as in CFS. BTW Roche has the definitive PCR test for mycoplasma. Often poor PCR tests will miss it.
As to Dr. Lo his work on mycoplasma is fascinating and confounding. I hope he continues to work on this murine retrovirus mystery. Have you read his original findings of mycoplasma fermentans (incognitus strain)? I don't know that the study is online. I should post it on my website. It describes six dead bodies brought to his lab. He determines that they all died in about 6-8 weeks from a virus-like infection. The only ones who lived a few more weeks were put on antibiotics. When they were taken off the antibiotics they ALL DIED. It turned out the virus-like infection was mycoplasma incognitus. I'd say this is not an infection you want to carry.
I have mycoplasma incognitus. How come I am still alive? Go figure. There are a lot of mysteries about CFS, aren't there?
>@AnonymousNonRetrovirologist
"antibodies can broadly cross-react and/or be selectively reactive (why will an antibody work fine in a Western, for example, yet fail when used in ELISAs?); "
The SU protein of SFFV can only react to an MLV non endogenous virus. MLVs attack dendritic cells which ELISA assays use.
"it looks like a little MLV can go a long way, witness 22RV1 cell line shedding replication-competent virions unbeknownst and undetected for years in many labs "
Did you mean to say MLV or MRV? No evidence exists that 22Rv1 is infected with anything but VP62.
"we have the still-never-quite-answered questions regarding the "non-germane" use of 5-AZA"
AZA was not germane as the reviewer and Science had the labels changed and removed the use of AZA. Are you blaming failure of the peer review to include that non german info or do you realise why AZA was not germane?
"And an EM can show nascent virus, fine, but in light of what has been revealed, can your EM image determine if the particle is an emergent infectious endogenized XMRV replicating within host, or an XMRV sourced from contamination (low sequence diversity, identical integration sites), or something else (ancient HERVs?) "
The EM is of a gamma retrovirus and the same size of an MLV, the virion is also budding/maturing from the cell. To be maturing the virion had to have been integrated. So it cannot be an endogenous virus or a contaminant.
"Sorry, must have missed that particular thread. "Safe" as in "personal safety"? Or "safe" as in "not jacking up your career"?
Not the later safe is it.
"Back in the 1980's I spent the better part of two years all garbed up like "Andromeda Strain" in a BSL3+ facility (…) It looks like XMRV is handled quite adequately by our innate immune systems, so unless immunocompromised, XMRV is probably not a dire infectious threat (and even so, it's not detected in HIV patients, for example)."
So now you admit XMRV is infecting people for it be causing an immune response! Who is using BSL3 to study MLV-related viruses? That would indicate a greater risk for infection.
"Dr. Mikovits should have just moved on without the cloak-and-dagger intrigue now alleged in Max Pfost's affadavits. And as a general rule, it's probably not a "safe" career move to steal stuff, even stuff that may legitimately be yours, from your ex-employers, especially if your ex-employers are rich and powerful, very well-connected and very unhappy with you."
The affidavit taken without a lawyer present and no miranda rights having been read that can be taken apart within minuets? No court case has ended and no one found guilty of materials who's ownership is now tied to a civil case.
>"And, of course, the ironic thing is that, by having been published in the literature, isn't this very work now at risk of being itself a false finding?"
That is always possible, but you are not oblivious to all the times this has been uncovered?
>Dr. Mikovits seems to be in good hands with her new lawyer, Scott Freeman.
Maybe folks could send letters in her behalf to him.
The courts have to decide this case.
>wow… There are way too many people on this blog that actually think they now what they are talking about.
"The SU protein of SFFV can only react to an MLV non endogenous virus. MLVs attack dendritic cells which ELISA assays use."
Two false statements. SU protein can't react to anything except the cellular receptor to which its binding. Maybe you meant the SU antibody? If you did then this is also false. An SU antibody primarily reacts with the SU protein of SFFV and can cross react with other SU proteins. This includes MLVs. MLVs attack dendritic cells? Of what? Humans? MLVs are specific to mice, did you mean polytropic or amphotropic? Any cell that has the receptor for MLV will be infected. Dendritic or not. Also, its false that ELISA assays use dendritic cells. ELISAs are non-cell based assays.
"To be maturing the virion had to have been integrated. So it cannot be an endogenous virus or a contaminant."
VERY FALSE. A retrovirus only becomes mature once it has bud from the cell and cleaved Gag polyprotein forming a capsid shell. Integration is not required for this. For example, in the lab I can transfect cells with plasmid DNA encoding the virus, express viral proteins and DNA, and get fully formed MATURE virions. No integration needed.
"So now you admit XMRV is infecting people for it be causing an immune response! Who is using BSL3 to study MLV-related viruses? That would indicate a greater risk for infection."
Any virus that infects humans or any mammal would cause an immune response. The fact remains that the immune system can clear and control the infection nicely. Immunodeficient patients however is another story.
Jamie, although as retrovirologist I disagree with your hypothesis, everyone is entitled to his or her own theories. Thats science.
However, you should seriously consider removing posts that clearly are false and misleading when describing basic facts of retrovirology. Maybe even the posts that are actually right as well (such as mine). Your readers are getting mistaken information.
>"SU protein can't react to anything except the cellular receptor to which its binding. Maybe you meant the SU antibody? If you did then this is also false. An SU antibody primarily reacts with the SU protein of SFFV and can cross react with other SU proteins. "
I meant to say the antibody to SFFV will only react with the SU protein of a MLV virus. So it won't react with mouse DNA or any ERV. What are you suggesting it could possibly be cross reacting with?
" attack dendritic cells? Of what? Humans? MLVs are specific to mice, did you mean polytropic or amphotropic? Any cell that has the receptor for MLV will be infected. Dendritic or not. Also, its false that ELISA assays use dendritic cells. ELISAs are non-cell based assays."
Gamma retroviruses infect follicular dendritic cells. Dendriatic cells are compromised by gamma retroviruses. Result – immune response cannot be maintained. An ELISA will need dendriatic cells to be functioning.
"VERY FALSE. A retrovirus only becomes mature once it has bud from the cell and cleaved Gag polyprotein forming a capsid shell. Integration is not required for this. For example, in the lab I can transfect cells with plasmid DNA encoding the virus, express viral proteins and DNA, and get fully formed MATURE virions. No integration needed."
If you look at this EM you can see a group of three virions top right. The virion to the bottom right of the three has an immature core. It is maturing. You can see the core forming. That cannot be a contaminant as it had to be integrated.
http://www.nih.gov/researchmatters/june2011/06132011XMRV.htm
"Any virus that infects humans or any mammal would cause an immune response. The fact remains that the immune system can clear and control the infection nicely. Immunodeficient patients however is another story."
Therefore MLV-related viruses are infecting people. Where is there evidence that the immune system clears the virus or that ME or prostate cancer patients are immunodeficient? ME patients are known to have overactive immune systems.
"However, you should seriously consider removing posts that clearly are false and misleading when describing basic facts of retrovirology. Maybe even the posts that are actually right as well (such as mine). Your readers are getting mistaken information."
Yes, your post should be removed if that is the standard.
>"I meant to say the antibody to SFFV will only react with the SU protein of a MLV virus."
Again NOT TRUE. Antisera against spleen focus forming virus (SFFV) *should* only react with protein of SFFV. If the proteins of MLV, or an ERV, are similar enough to SFFV (which it is), then yes it could cross-react. That's why not many people in the research trust polyclonal antibodies used for immunohistochemistry purposes.
" Dendriatic cells are compromised by gamma retroviruses. Result – immune response cannot be maintained. An ELISA will need dendriatic cells to be functioning. "
Did you not read my last statement? An ELISA DOES NOT USE CELLS!! lol… And no, mammalian type c retroviruses (not HIV) do not compromise dendritic cells. Show me the paper where they do and you've got me.
"If you look at this EM you can see a group of three virions top right. The virion to the bottom right of the three has an immature core. It is maturing. You can see the core forming. That cannot be a contaminant as it had to be integrated."
I gave Ila the plasmid to generate that virus!!! Trust me, its not from integrated provirus. Those virions came from 293T cells transfected with VP62 plasmid.
"Therefore MLV-related viruses are infecting people."
Show me the proof… None exists so far. As for clearing the infection, Silverman's animal study proved this very well.
Jamie, please bar all comments with shoddy scientific reasoning. I implore you.
>"Again NOT TRUE. Antisera against spleen focus forming virus (SFFV) *should* only react with protein of SFFV. If the proteins of MLV, or an ERV, are similar enough to SFFV (which it is), then yes it could cross-react. That's why not many people in the research trust polyclonal antibodies used for immunohistochemistry purposes."
Completely wrong. This is what Sandra Ruscetti has been studying for 40 years. It cannot detect ERVs. Think about it for a moment. I'm sure you can do that much. Do you realise you have said it cannot react with anything and then that it can but only to MLVs? Try not picking and choosing and instead read. It will only detect a human immune response to MLV virus.
"Did you not read my last statement? An ELISA DOES NOT USE CELLS!! lol… And no, mammalian type c retroviruses (not HIV) do not compromise dendritic cells. Show me the paper where they do and you've got me."
You didn't read mine. Gamma retroviruses compromise the immune response because they attack dendriatic cells. I notice how you choose to ignore FISH and IHC, which have been used to detect these viruses. Are you really incapable of doing a search? lol
"I gave Ila the plasmid to generate that virus!!! Trust me, its not from integrated provirus. Those virions came from 293T cells transfected with VP62 plasmid."
So we should know who you are then! The virion is maturing. You can see the core forming. Any one with eyes can. What does it matter who you gave something to. Dr Ruscetti has stated that this is evidence that this is not contamination at a conference only this year. Did you know 293T cells are infected with XMRV?
"Show me the proof… None exists so far. As for clearing the infection, Silverman's animal study proved this very well."
You admitted it. "Any virus that infects humans or any mammal would cause an immune response." You don't seem to want to tackle any other issues I have raised.
"Jamie, please bar all comments with shoddy scientific reasoning. I implore you."
Who are you?
>"XMRV is present in malignant prostatic epithelium and is associated with prostate cancer, especially high-grade tumors
Robert Schlaberga,1, Daniel J. Choeb, Kristy R. Browna, Harshwardhan M. Thakerb and Ila R. Singha,b,2"
"We constructed pXMRV1, a full-length XMRV molecular clone, using 2 overlapping clones from patient isolate VP62 (6) [gift of Don Ganem, University of California, San Francisco (UCSF)]."
"Particles released from XMRV-infected cells closely resembled those of a gammaretrovirus, Moloney murine leukemia virus (MoMLV), in size and morphology (Fig. 1 B–E). "
>" As for clearing the infection, Silverman's animal study proved this very well"
Clear the infection!!! Is that all you have to say. Granted monkeys are not like humans and this is artificial inoculation with an artificial virus, but what did they show.
Onlamoon
"“The virus causes chronic, persistent infection,” says Robert Silverman of the Cleveland Clinic, a co-author of the paper, which was published online yesterday in the Journal of Virology. Moreover, the new research suggests that in these monkeys, at least, the virus can be difficult to detect in blood, even though it’s taken root in the body." http://blogs.wsj.com/health/2011/02/17/xmrv-study-shows-virus-can-cause-persistent-infection-in-monkeys/
"Of note, in spite of the intravenous inoculation, extensive XMRV replication was noted in prostate during acute but not chronic infection, even though infected cells were still detectable by FISH in prostate at 5 and 9 months post infection. Marked lymphocyte activation occurred immediately post infection, but antigen specific cellular responses were undetectable. Antibody responses were elicited and boosted upon reexposure, but titers decreased rapidly suggesting low antigen stimulation over time. Our findings establish a nonhuman primate model to study XMRV replication/dissemination, transmission, pathogenesis, immune responses, and potential future therapies."
"However, the titers to XMRV antibodies rapidly decreased to a low level even after the second infection, indicative of a lack of sustained antigen stimulation of humoral responses, either due to poor release of XMRV from infected cells or the presence of immunosuppressive mechanisms (34)."
http://jvi.asm.org/content/early/2011/02/16/JVI.02411-10.abstract
>Oh and Onlamoon had this to say about the techniques used in the study and in the paper where prostate cancer XMRV was discovered.
" Furthermore, the results presented herein, only marginally relied on amplification techniques with the majority of the data generated by techniques that do not involve PCR, were not susceptible to contamination errors and were adequately controlled."
>Lab Invest. 1995 Oct;73(4):511-20.
Loss of follicular dendritic cells in murine-acquired immunodeficiency syndrome.
Masuda A, Burton GF, Szakal AK, Tew JG.
Source
Department of Microbiology and Immunology, Virginia Commonwealth University, Richmond, USA.
Abstract
BACKGROUND:
The disease caused by HIV-1 leads to the destruction of follicular dendritic cells (FDC) and the follicular architecture in secondary lymphoid tissues. The murine acquired immunodeficiency syndrome (MAIDS, caused by LP-BM5) serves as an animal model for study of mechanisms involved in development of retrovirus-induced immunodeficiencies. The present study was undertaken to determine whether LP-BM5 infection leads to the destruction of murine FDC and the normal follicular architecture in secondary lymphoid tissues.
EXPERIMENTAL DESIGN:
Mice were infected with LP-BM5, and the follicular architecture and FDC networks were assessed. The pathologic changes observed were correlated with FDC function.
RESULTS:
Three weeks after infection, FDC networks were present, and they often appeared hyperplastic. However, by 1 month after infection, distorted lymphoid follicles were apparent, and the intensity of FDC labeling began to decline. FDC disappeared first in the spleen, and in hyperimmunized mice, FDC in draining lymph nodes disappeared before FDC in nondraining lymph nodes. By 4 months, the normal follicular localization of B cells was missing, and FDC were not detectable in most tissues. As the FDC and the normal lymphoid architecture degenerated, extrafollicular foci of immunoblasts and plasma cells appeared in areas typically reserved for T cells, and the Thy 1.2+ T cells were dispersed. Of interest, the total number of Ig-producing cells increased as the disease progressed; in contrast, the number of anti-human serum albumin-producing cells in mice immunized with human serum albumin before infection decreased.
CONCLUSIONS:
These data indicate that, like HIV-1 infection, LP-BM5 infection leads to the loss of FDC and the normal follicular architecture. However, morphologic changes were not observed until after FDC had lost their normal ability to trap and retain Ag. These data indicate that retroviral infections may cause FDC dysfunctions long before FDC are destroyed.
>Anon @ 10:31 AM
It is clear to me that you do not do research, nor are you educated in the finer points of retrovirology.
" It cannot detect ERVs."
This is what I'm saying – it can. Believe me or not, I don't care. All I know is not many scientists trust IHC staining using a polyclonal antibody because it detect multiple things other than MLV. This inlcudes ERVs from mice and humans.
"Gamma retroviruses compromise the immune response because they attack dendriatic cells."
Again, show me the paper and I'm a believer. I'm all ears.
"So we should know who you are then! The virion is maturing. You can see the core forming. Any one with eyes can."
Of course it can and is mature!! This is not what I'm disagreeing with you about. You stated that the virus needs to be integrated to mature. THIS IS NOT TRUE. Good lord.
"Did you know 293T cells are infected with XMRV?"
Sigh. 293T cells are not infected unless they are purposefully infected with virus. Actually, XMRV doesn't replicate in 293T well at all. HOWEVER, if you put a plasmid in 293T that expresses the virus, virus will come out from those cells. What is so hard about this?
"You admitted it. "Any virus that infects humans or any mammal would cause an immune response." You don't seem to want to tackle any other issues I have raised. "
Of course! You get a cold and you get a immune response. Sure the same is true for XMRV or any other virus, real or made ten years ago in a lab. As for your statement:
""Therefore MLV-related viruses are infecting people.""
Show me the proof! This is quite different from starting an immune response. Besides the now-debunked Mikovits paper, there is ALter and Lo. Personally, I'm not convinced of it yet as they need more controls to rule out HERVs that populate our genomes.
"Who are you?"
HA!!!! You expect me to reveal my identity so other scientists can be ridiculed and burned at the stake (so to speak) on this blog? Like Coffin/Stoye/Jason?
Pfftt… Yeah right.
>"Lab Invest. 1995 Oct;73(4):511-20.
Loss of follicular dendritic cells in murine-acquired immunodeficiency syndrome."
OK, now we are onto something.
I'll give it you that for this particular MLV, DCs seem to have a problem.
However, it also possible that lots of other things are going in the immune system during the infection that can cause a drop in DCs.
The authors of that paper never proved that the virus ITSELF is attacking DCs, just that DCs are dropping. Similar to other cell types.
I'm sure this explanation will satisfy no one.
>@Retrovriologist
"This is what I'm saying – it can. Believe me or not, I don't care. All I know is not many scientists trust IHC staining using a polyclonal antibody because it detect multiple things other than MLV. This inlcudes ERVs from mice and humans."
The monoclonal antibody to SFFV is specific to MLV SU proteins. It will not react with ERVs. Come on I asked you to think about it.
No the IHC test was shown not to detect mouse ERVs. The staining occured in tissue taken from prostate cancer sufferers and at a density of 1 cell in 660 counted. Staining did not occur in healthy tissue and gammaretroviral HERVs are the only possible other candidates. If this was an issue all of the tissue samples would have been stained in all cells and not 22% of tissues examined. The belief that this test could detect ERV or HERV proteins is bunkum.
"Again, show me the paper and I'm a believer. I'm all ears."
Did do.
"Of course it can and is mature!! This is not what I'm disagreeing with you about. You stated that the virus needs to be integrated to mature. THIS IS NOT TRUE. Good lord. "
It is not mature, the core is forming. Frank Ruscetti used this as an example only in the last few months and said that was proof it was not contamination because it is immature. A retrovirus cannot make proteins if not integrated, so virions would not assemble. Maturation occurs post budding.
"Sigh. 293T cells are not infected unless they are purposefully infected with virus. Actually, XMRV doesn't replicate in 293T well at all. HOWEVER, if you put a plasmid in 293T that expresses the virus, virus will come out from those cells. What is so hard about this?"
Yes, that is possible, same as for 22Rv1, which has not been shown to be infected by anything but VP62. Take this from a forthcoming abstract. They say "contaminated", but they need to provide proof of that. These cells predate 22Rv1 by 15 years even if 22Rv1 had ever been shown to be contaminated.
"XMRV sequences obtained from 22Rv1 and XMRV-contaminated 293T cell-lines."
http://antiviralresistance.org/abstract26_2011.pdf
"Of course! You get a cold and you get a immune response. Sure the same is true for XMRV or any other virus, real or made ten years ago in a lab."
Therefore patients are infected with MLV-related viruses, which is what you said. No evidence has been published to argue against Lombardi or Lo et al. The negative papers did look for the wrong virus, and optimised to a synthetic strain that no one has found. They also failed to clinically validate. There is also no evidence of contamination in any of those papers. Plenty of rhetoric, but no evidence.
"HA!!!! You expect me to reveal my identity so other scientists can be ridiculed and burned at the stake (so to speak) on this blog? Like Coffin/Stoye/Jason?"
You say you gave Singh the plasmid for Schlaberga et al? According to the paper Ganem provided that. So you could be an underling or an impostor. You do now realise that the EM is not of VP62 as there is no evidence that exists in nature.
As you can see ELISA assays not detecting a positive are not minus an explanation. Why! you are doing yourself out of a job making others think all and sundry can perform ELISAs, PCR, FISH.
>"The authors of that paper never proved that the virus ITSELF is attacking DCs, just that DCs are dropping. Similar to other cell types."
The paper was from 1995. Go on have a look at the later reserach.
>@ Retrovirologist,
Besides Jason, who took it upon himself to so quintessentially embody the broader problem, the scientists you mentioned were criticized by me (as opposed to commenters) for taking it upon themselves to practice medicine without licenses. I would never attack someone actually trying to engage the discussion in good faith. And you seem to be doing that. As I have said all along, I welcome honest disagreement; I have only criticized people for their closed minds, and for not considering the consequences their assumptions have on the health of patients directly. Do you know anything about the pathophysiology of the disease under discussion? Autism? Part of the problem we are having is that the scientists involved know nothing about the disease. If they did, they would be more excited. Though I suspect some are very excited, though closeted at the moment.
"Any virus that infects humans or any mammal would cause an immune response."
The immune response seen in ME/CFS is much more specific than that, and more consistent with the persistent immune activation which has been studied in HIV disease.
Innate immune recognition and activation during HIV infection
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2904714/?tool=pubmed
Xenotropic Murine Leukemia Virus-related Virus-associated Chronic Fatigue Syndrome Reveals a Distinct Inflammatory Signature
http://iv.iiarjournals.org/content/25/3/307.long
The MLV literature gives us a model of microglial activation with loss of endothelial integrity and support for clonal expansion that fits the clinical picture well. The variation in specific pathogenesis from one MLV to another seems consistent with what we see clinically, variations on a theme, consistent with my theory that it isn't one virus, but many, introduced at various times in vaccines (and other less important ways) and subject to recombination events over time.
Importance of macrophage inflammatory protein-1α and splenic macrophages in neurodegeneration induced by PVC-211 murine leukemia virus.
http://www.ncbi.nlm.nih.gov.ezlib.ncifcrf.gov/pubmed/21051067
Immunologic havoc induced by the 60 kD Gag protein of the MAIDS defective virus.
http://www.ncbi.nlm.nih.gov/pubmed/9209332
Defective T cell receptor-mediated signaling and differential induction of T cell functions by murine AIDS virus superantigen.
http://www.ncbi.nlm.nih.gov/pubmed/8382246
In addition, there are many other clues. Methylation block, mitochondrial defect, patterns of inheritance and epidemiological evidence.
Warmly,
Jamie
P.S. Thank you for participating.
>Dr. D-J,
I look forward to your report on the informal survey re history of onset. In particular I will be curious to note who got vaccines prior to onset. I was given routine vaccinations about the timeframe I started getting sick, because I was going to spend a week in a rural area of Mexico. I wonder how many of us fit this picture?
>I only got vaccinations as a young child, before there were vaccines against measles, mumps, and chicken pox. I got those diseases and also roseola.
In later grades in grammar school, I got the Salk vaccines against polio.
Then at the end of high school, I got a bad case of mononucleosis.
Before I got CFS, I got a bad case of the flu every winter for about four years in a row, would be home from work sick for 1 1/2 weeks, and then drag around without energy for 2-3 months. Then the final bout never ended. Then I had CFS, as so diagnosed by my good doctor.
>News today that Dr. Nancy Klimas is opening up a neuro-immunological center at Nova Southeastern University in Florida, which will specialize in ME/CFS and GWI.
Research will be part of it and it will have a clinical part also.
>Every Klimas paper I have read doesn't use a definition that requires neurological signs and symptoms. Combining cohorts this way explains why her immune profile looks like depression.
>Retrovirologist,
I have some general, broad questions which may appear simplistic, but I think get to the heart of the issues we face:
1. What was different in the procedures used in the labs who found no evidence of a murine retrovirus contrasted with the labs who found some positives?
2. Why would labs who found some form of a murine retrovirus (Mikovits, Lo, Silverman in prostate cancer) not find the lab contaminant in every sample, if it was a lab contaminant?
****Curious note on the prostate cancer cases – these were men with a genetic problem of low RNASEL which is also found in CFS patients – see DeMeirleir research on this.
3. What significance would you give to Mikovits' growing cultures of and finding antibodies to the retrovirus she found? Would this be possible to do if it were a lab contaminant?
3. Relevant to this third question is the research which indicates that lab contaminants of XMRV type viruses are highly contagious to human tissue. Given this, what if at this stage in the research we are seeing both humans already infected with a murine retrovirus AND lab contamination, possibly from those human blood samples and not from the reagents used to test?
bit.ly/pdrEpU
The high susceptibility of human cells to
> infection with XMLV, the high levels of
> reverse transcriptase activity present in
> culture supernatant fluids and the
> demonstrated infectivity of the shed
> virions suggest that such viruses may
> present potential biohazards to laboratory
> personnel involved in cell culture facilities
> or to those handling human xenografts.
>Clinical validation is not being used by negative studies. There assays can be said to be real cause for failing to find a positives for human gamma retroviruses.
http://www.genomeweb.com/sites/default/files/pdfs/genomeweb/GenomeTechClinGenotypingTechGuide.pdf
"Blinded samples from another laboratory performing the same assay or assay type will be tested to confirm sensitivity and specificity of previous testing results.”
— Betsy Bove
"We use negative and positive controls at all steps as a matter of routine. Our lab serves as a reference lab for collaborating labs, so when they have a novel or unexpected result, they will send us blinded samples and we repeat the genotyping with no knowledge of their results. Discrepant results are repeated and confirmed by sequencing, preferably from the original clinical sample rather than extracted DNA."
— Christopher Plowe
>The assays they are using are not clinically validated, which leaves the lab technicians in a terrible predicament. Keep quiet and let this happen and risk your health and that of your family, or speak out now.
BASHAM: "…I'm a little concerned, you know one this was human created through… in the laboratory and it's a highly infectious retrovirus and could it transmit to humans. Could it have subsequent to the event transmitted to humans. We've been doing studies using pedigreed negative controls, some of whom happen to be lab workers who are working with this virus who intermittently score positive in one lab or another and I've just ignored that but now I'm beginning to be a little concerned that might there be transient infections of humans. Has anyone embarked on studies to look at either nucleic acid or serologic detectability in lab workers who have or are working with these cell lines and ex-cetera?"
JONES: "I do know of some animal studies where the lab handlers are being monitored. I don't think anyone in the laboratory is…there's ethical reasons I think not to test each other."
STOYE: "One, I can talk about an anecdote among urologists in Britain who were suddenly alarmed that this cell line that they had been using was loaded with virus. I think there are some of us that have been working with XMRV or related viruses for… well I have been doing it for 35 years or something, and I know I'm negative or at least I was the last time I looked."
SWITZER: "I just wanted to add to that, we share your concern Mike and we have started a study looking at some archived specimens that we have from laboratory workers that we screened and found other simian retroviruses in for example, that we are going to look for XMRV evidence of other MuLVs."
CROI 18, March 2011
>@Paula
Answers to your questions.
1. What was different in the procedures used in the labs who found no evidence of a murine retrovirus contrasted with the labs who found some positives?
-Different assays used and failure to clinically validate the assays used in the negative papers.
2. Why would labs who found some form of a murine retrovirus (Mikovits, Lo, Silverman in prostate cancer) not find the lab contaminant in every sample, if it was a lab contaminant?
****Curious note on the prostate cancer cases – these were men with a genetic problem of low RNASEL which is also found in CFS patients – see DeMeirleir research on this.
-The genetic defect was later found to not be necessary for a prostate cancer patient to be infected with XMRV. No evidence exists to suggest this is contamination. The dramatic difference in patients versus controls is supporting evidence against contamination as both Lo and Lombardi were blinded studies.
3. What significance would you give to Mikovits' growing cultures of and finding antibodies to the retrovirus she found? Would this be possible to do if it were a lab contaminant?
Yes, you can grow a contaminant, but you cannot produce an immune response for one or take an EM of a maturing virion.
3. Relevant to this third question is the research which indicates that lab contaminants of XMRV type viruses are highly contagious to human tissue. Given this, what if at this stage in the research we are seeing both humans already infected with a murine retrovirus AND lab contamination, possibly from those human blood samples and not from the reagents used to test?
An assay not only needs to be capable of detecting the virus but also needs to be controlled for contamination. It may seem obvious but not all labs used have never worked with mice and many have found they had mouse contamination in their samples. However these viruses are human viruses and this was not found to be the reason for the positive studies. The positive studies used labs that had never worked with mice and have never found mouse contamination.
Many labs and the blood working group, despite the claims that 22Rv1 is infected and easy to contaminate, also continue to use this cell line to analytically validate their assays, but this step still does not provide clinical validation as it only shows an assay is detecting an artificial virus spiked into blood.
A positive human sample could become infected in the lab with a contaminant and only the contaminant be detected because an assay is not optimised to the wild-type virus. We also need to consider that despite claims that VP62/XMRV was created in a lab by accident, this is not the only MLV-related virus that is being discovered in people. Not all variants and strains need to have been lab created or jump to humans through zoonosis. It is easy to see how not having known about these viruses infecting human cells new variants may have been created and entered the population. Without fully sequencing each positive, it is not possible to know what the strain or variant is.
>Hi, Jamie.
You may already be well aware of this, but your mention of C4a, TGFbeta-1, and Marfan's syndrome is very reminiscent of the things that Dr. Ritchie Shoemaker talks about in connection with biotoxin illnesses. His recent seminar in Santa Rosa, CA, sponsored by Gordon Medical Associates, including interpretation by Dr. Neil Nathan, was a fairly well organized presentation of his thinking. The syllabus is available from http://www.gordonmedical.com, and Scott Forsgren has posted a fairly detailed report on his blog at http://betterhealthguy.com/joomla/blog/251-biotoxin-illness-conference-2011
Best regards,
Rich Van Konynenburg
>Rich, Thanks so very much for a nice, concise reply. I hope "retrovirologist" will be reading and also comment. Have we oversimplified? If so, in what areas? What might we be missing?
Do you think the RNaseL issues in CFS are also a moot point?
I have missed the conferences of late – busy doing other things for my own health and enjoying family. Keep up your good work!
>To read more on the Dr. Klimas good news: http://forums.phoenixrising.me/content.php?513-Klimas-to-Form-Neuro-Immune-CFS-ME-CFS-Institute-at-Nova-Southeastern
>I thought the same, refreshing update. Interesting to hear what you're doing in practice.
For a while I've suspected hypermobility correlates with neuroimmune illness, based on my personal experience. I am guessing it's a chicken and egg situation with the two. Both causal and affected by.
@Paula – Many of us were exposed to foreign viruses during international travel, a partner who travelled. In my opinion, it increases the odds of getting some intractable virus.
>@Amy
"In my opinion, it increases the odds of getting some intractable virus."
What does?
Thanks
>"Moreover, the new research suggests that in these monkeys, at least, the virus can be difficult to detect in blood, EVEN THOUGH IT'S TAKEN ROOT IN THE BODY.""
I just liked that quote so much I had to repeat it. In caps.
:)
My regards to Retrovirologist.
>Hi Paula,
Sorry for the delayed response, but work has been keeping me busy. Great questions by the way and I'll attempt to answer them to the best of my ability. However, keep in mind that the questions you answered have grey areas that are subtle and complex, which may lead to no clear cut answer.
Also, one other thing. Take Anon @ 1:00pm comments with a grain of salt. He does not appear to a professional or someone in research, but rather someone with an agenda. Much of what he wrote (not everything) has fallacies.
OK here we go:
1. What was different in the procedures used in the labs who found no evidence of a murine retrovirus contrasted with the labs who found some positives?
The tricky answer is the were both different and the same. I know this is frustrating but this is the way science does something. For example, two labs could run a nested PCR as the same procedure but the parameters could be different. Or the samples could be isolated differently. Another reason could be using different antibodies to detect MLVs, again same technique but different reagents. Generally, this is a good thing. If a finding is held to true, it must be repeated, but not just exactly. If ten labs look at a finding in slightly different ways, some might be looking at it with poor resolution, some with great resolution. At some point, a finding (if true) will get replicated. This is how science works most of the time. Now for XMRV, some labs used the exact same protocols as Mikovits and did not find anything. Some labs, from what I gather, had even better resolution (in technique) and also couldn't find anything. So in summary, it doesn't matter so much if small things in technique differ. But what does matter is that if something is true, it should be able to repeat. Multiple times. This is why research proceeds at snails pace much to the patients chagrin.
2. Why would labs who found some form of a murine retrovirus (Mikovits, Lo, Silverman in prostate cancer) not find the lab contaminant in every sample, if it was a lab contaminant?
****Curious note on the prostate cancer cases – these were men with a genetic problem of low RNASEL which is also found in CFS patients – see DeMeirleir research on this.
A lab contaminant does not necessarily have to contaminate every sample. There are so many variables that are left to chance for stuff like this to occur. For example, on the day when Don Ganem and his lab were scraping the wells from their Virochips from RNASEL mutant samples, maybe someone was working with 22Rv1 (or other contaminated line). This scenario is exceedingly rare, but possible? Sure. As for the Lo paper, it is clear he found something as he rules out murine mitochondrial DNA contamination. Those sequences are closely related to PMLVs and no one has tried to repeat the Lo results. This could prove to be interesting, but more work needs to be done. As for the RNASEL connection I personally remain unconvinced. RNASEL is an antiviral gene whose function is to virus infection by destroying viral RNA. At the same time, it kills the cells by apoptosis to prevent further infection. In the original study RNASEL has a mutation that only partially inactivates it, not totally. In my opinion, if RNASEL was that important, why didn't they find other viruses? Also, the connection of RNASEL and CFS is tenuous at best and I can expand on this further if you like.
continued…
>3. What significance would you give to Mikovits' growing cultures of and finding antibodies to the retrovirus she found? Would this be possible to do if it were a lab contaminant?
Some possibilities here. One is the very unfortunate possibility that she committed scientific fraud. Just figured I'd get that one out of the way first (which may not be true). Onto the others. It appears that she definitely grew some sort of retrovirus. Just in case you are not aware of how the assay (in figure 4D) works I'll explain it. Basically, BaF3ER cells is a monoclonal B-cell line that produces the env protein of spleen focus forming virus (SFFV). When you mix those cells with a solution that has antibodies to SFFV env then the cells light up and this can be measured. The problem is the specificity. The experiment ASSUMES that antibodies to XMRV cross react with another murine retrovirus. Whether you believe this data or not depends on similar you think XMRV and SFFV really are. As answer to your second part, I would have to say no, a lab contaminant (XMRV) that infected PBMCs and made antibodies would be VERY rare. However, there is another possibility. The sera from those patients have made antibodies to SFFV, not XMRV.
3. Relevant to this third question is the research which indicates that lab contaminants of XMRV type viruses are highly contagious to human tissue. Given this, what if at this stage in the research we are seeing both humans already infected with a murine retrovirus AND lab contamination, possibly from those human blood samples and not from the reagents used to test?
You know, I'm not so sure that XMRV as a lab contaminant is very infectious. XMRV has clearly been shown to love prostate cells but not others. I think the jury is still out on that question. The reason I'm leaning towards less infectious is because the lab contaminant that is known as XMRV (this has been proven very conclusively) has not been found in many studies that have looked for it. As for other murine retroviruses that have made the jump in the species barrier to humans I think its possible, sure. However, research needs to be done bear this out. Specifically, I would like to see more studies looking for PMLVs in humans. Also, I definitely know that Lipkin is continuing to look for retroviruses in CFS samples as well.
Hope this helps.
>"Moreover, the new research suggests that in these monkeys, at least, the virus can be difficult to detect in blood, EVEN THOUGH IT'S TAKEN ROOT IN THE BODY.""
I just liked that quote so much I had to repeat it. In caps.
:)
My regards to Retrovirologist.
You know I'm glad that you put that in caps, because its an important point. Specifically, TAKEN ROOT.
What I mean by clearing the virus means clearing viremia. Clearing the blood/body if virus particles. This clearly happens in these monkeys. By the immune system. However, the virus TAKES ROOT because it is a retrovirus and integrates in the host DNA, continuing to express viral protein. Therefore you can detect it in the blood, although there might not be any virus particles left.
>Retrovirologist,
I look forward to reading all of your thoughts on this. I think anon @1 is a PhD but not a retrovirologist, if this is the person who posted earlier and now the name is missing.
One more notion to pass along. This pertains to RNaseL and CFS and comes from Kenny DeMeirleir's book on CFS chapter 10. This is a brief section of Cort Johnson's summary. I would encourage you to read the book as it may shed light on what is going on in CFS.
A Laymen's Guide to Chapter Ten of Chronic Fatigue Syndrome
A Biological Approach by Cort Johnson
CHRONIC FATIGUE SYNDROME A BIOLOGICAL APPROACH
Edited by Patrick Englebienne Ph.D., Kenny DeMeirleir M.D,
Ph.D., CRC Press. Washington D.C. 2002
"RNase L, 2-5OAS and PKR are all upregulated in CFS.
Levels of 2-5A, the adenylate oligomer produced by 2-5OAS that
binds with RNase L, are high as well. The evidence suggests,
however, that an abnormal form of 2-5A that is produced in CFS
patients, is long enough to bind with RNase L, but is too short to
induce it to dimerize (and become activated. High levels of this
discordant RNA will therefore end up inhibiting the activity of the
native RNase L. The upregulated RNase L activity found in CFS
is must, therefore, primarily (but not completely) be due to poorly
regulated 37-kDa fragment? Or does 2-5OAS produce both long
and short forms of 2-5A? If this is so, the high RNase L activity
could be due to both the native and the fragmented RNase L
could be high. Some evidence supports this model. Apoptotic
activity, possibly induced by the native RNase L, is high during
the first stages of RNase L fragmentation, and then decline as
the fragment becomes more and more abundant. In the best of
times and healthiest of patients 2-5OAS produces a mixture of
oligomers – including those too short to induce RNase L
dimerization. This is why the 37kDa fragment can be detected in
health controls. ) RNase L remains in a monomeric form that is
susceptible to cleavage by proteolytic enzymes. Once apoptotic
and/or inflammatory occurs, the native RNase L is broken up
and the 37-kDa fragment is generated.
(The central question then is why does 2-5OAS produce 2-5A
oligomers (dimers) that are not only too short to induce RNase L
to dimerize but actually inhibit RNase L activity and leave it open
to fragmentation?) The authors report that 2-5OAS induction by
type I IFN's is a `very sensitive, tightly regulated process'. It
requires protein kinase C (a kinase we have not come across
before) and multiple regulatory elements that are either activated
or repressed by interferon regulatory factors 1 or 2. 2-5OAS only
produces oligomers long enough to induce RNase L
dimerization if the pieces of ss or ds RNA are `aptamers' `with
little secondary structure' or if the dsRNA is over 25 bp's long.
That the 2-5OAS system works properly in CFS patients
undergoing Ampligen therapy suggests that the activators not
the system are impaired in CFS. (Ampligen is an engineered
dsRNA that properly activates the 2-5OAS system.).
The different viruses found in the CFS patient population
could provide the triggers for the abnormal 2-5OAS response.
(This very interesting statement broadens the search for the
cause of the poor 2-5OAS inducers. Any of the viruses found in
CFS could do it! It begs the question, however, why viral attack
would produce small or oligo deficient RNA in a person with CFS
and not in one without it. This appears to push us to look ever
more closely at the viral response. Just how does dsRNA
appear in the cytosol? Just how are the viral metabolites that
turn on the IFN system created? Is there a problem with the
phagocytic processing in monocytes/macrophages?) The
authors suggest that endogenous retroviral sequences that are
part of our genome or short interspersed elements that contain
`ALU' sequences, could also be poor 2-5OAS inducers."
>@retrofraud
"Another reason could be using different antibodies to detect MLVs, again same technique but different reagents. Generally, this is a good thing. If a finding is held to true, it must be repeated, but not just exactly. If ten labs look at a finding in slightly different ways, some might be looking at it with poor resolution, some with great resolution. At some point, a finding (if true) will get replicated. This is how science works most of the time. Now for XMRV, some labs used the exact same protocols as Mikovits and did not find anything."
Replication is a fundamental of the scientific method. A hypothesis is impossible to dismiss without replication. When an assay uses different variables, it is a different assay. No other study has replicated the methodologies used by Dr Mikovits and Dr Ruscetti in Lombardi et al. None of these different assay have been clinically validated either.
Paula if you want evidence ask them to say what paper what assay. Then the differences can be highlighted again.
>Hi Retrovirologist,
"Specifically, I would like to see more studies looking for PMLVs in humans."
Where specifically is funding for this coming from, do you know?
Are you personally involved?
"Also, I definitely know that Lipkin is continuing to look for retroviruses in CFS samples as well"
That's good to hear. Do you have a reference?
Thanks.
>Anon 8:02 PM,
That was uncalled for. Retrovirologist is sharing his expertise generously with us and I welcome him. He is telling us what is real in his world. We all need meaningful discussion, not ad hominem attacks. Cease and desist; find a way to express your opinions politely.
Jamie
>"A lab contaminant does not necessarily have to contaminate every sample. There are so many variables that are left to chance for stuff like this to occur. For example, on the day when Don Ganem and his lab were scraping the wells from their Virochips from RNASEL mutant samples, maybe someone was working with 22Rv1 (or other contaminated line). This scenario is exceedingly rare, but possible? Sure. As for the Lo paper, it is clear he found something as he rules out murine mitochondrial DNA contamination. Those sequences are closely related to PMLVs and no one has tried to repeat the Lo results."
A lab contaminant should however contaminate in equal amounts. That did not occur in Lombardi or Lo.
The viruses detected in Lombardi and Lo cannot now be claimed to be different, as there is nothing xenotropic about the Lombardi viruses. They are like Lo's polytropic. These viruses have also never been shown to be the prostate cancer XMRV. Whereas the techniques used in the positive prostate cancer studies are not not prone to contamination and 22Rv1 has not been shown to be infected, only contaminated by VP62 that Silverman himself made in 2006.
>@Jamie, if he wants to claim he is a retrovirologists he should give his name. It's an appeal to authority and underhand.
>"You know, I'm not so sure that XMRV as a lab contaminant is very infectious. ".
Which kills any possibility that the positive studies are contamination without direct evidence.
" As for other murine retroviruses that have made the jump in the species barrier to humans I think its possible, sure. However, research needs to be done bear this out.".
The Lo and Lombardi findings are the same. Other MLV-related viruses have already infected and killed children when used in gene research. It has happened already. The reports can be found on pubmed and the FDA website.
>"What I mean by clearing the virus means clearing viremia. Clearing the blood/body if virus particles. This clearly happens in these monkeys. By the immune system. However, the virus TAKES ROOT because it is a retrovirus and integrates in the host DNA, continuing to express viral protein. Therefore you can detect it in the blood, although there might not be any virus particles left."
Gamma retroviruses preferentially propagate in tissue not blood and are hardly ever detected in blood. Without screening the compartments where these viruses do find their natural home a person cannot ever be declared to be negative. As these viruses also produce low titres again it is impossible to declare a person negative. PCR has its limits.
>"Also, I definitely know that Lipkin is continuing to look for retroviruses in CFS samples as well"
Use of assays not clinically validated or optimised to a synthetic viruses that does not mimic the viruses detected in people with ME means an assay will not work. An assay that does not work cannot then be used to screen people. Doing this on people suspected of having a HIV infection ends in a jail sentence.
>@Paula
RNaseL has no influence on who is infected with MLV-related viruses. This was proven in Singhs positive prostate cancer study, the one that used different assays to her ME study.
>"Some possibilities here. One is the very unfortunate possibility that she committed scientific fraud. Just figured I'd get that one out of the way first (which may not be true). Onto the others. It appears that she definitely grew some sort of retrovirus. Just in case you are not aware of how the assay (in figure 4D) works I'll explain it. Basically, BaF3ER cells is a monoclonal B-cell line that produces the env protein of spleen focus forming virus (SFFV). When you mix those cells with a solution that has antibodies to SFFV env then the cells light up and this can be measured. The problem is the specificity. The experiment ASSUMES that antibodies to XMRV cross react with another murine retrovirus. Whether you believe this data or not depends on similar you think XMRV and SFFV really are. As answer to your second part, I would have to say no, a lab contaminant (XMRV) that infected PBMCs and made antibodies would be VERY rare. However, there is another possibility. The sera from those patients have made antibodies to SFFV, not XMRV. "
Nice! Not true at all as you know. That is Dr Ruscetti you are accusing! Do you're you trying to stop spending on HTLV too?
SFFV will only react to the SU protein of an MLV. The experiment does not assume anything, it is built upon many research papers, including Sandra Ruscettis 40 year expertise on this very subject. It is also impossible to have an immune response to a contaminant.
Paula if you are really interested ask for a reference on what else SFFV could possibly be cross reacting with. Ask for a reference that shows contaminants cause an immune response. You won't get one.