
One morning an elderly man was walking on a nearly deserted beach after a big storm had washed up thousands and thousands of starfish. He came upon a boy who was picking them up and throwing them back into the ocean, as eagerly as he could.
Puzzled, the older man looked at the young boy and asked, “Little boy, what are you doing?”
The youth responded without looking up, “I’m trying to save these starfish, sir.”
The old man chuckled aloud, and queried, “Son, there are thousands of starfish and only one of you. What difference can you make?”
Holding a starfish in his hand, the boy turned to the man and, gently tossing it into the water, said, “It will make a difference to that one!”
It is all well and good to say that now that XMRV is dead, science can get back to its orderly, stepwise process; they even get to say, we told you so. And I say what I have said all along: millions of patients need treatment now. It is not a static situation. It is a progressive disease, slow, but lots of people are circling the drain. Many new cases that might be easier to treat sooner rather than later… that might respond more completely to arv’s. New babies being born with it. Should we wait a decade to start to find out, in a systematic way, if existing treatments might not affect it? It is incumbent upon the medical and pharmaceutical industries to think about the disease in concept and find solutions, not sit there doing nothing until Virus X is found; that approach already hasn’t worked for decades. It is quite likely that it won’t turn out to be a one virus, one disease, one treatment paradigm. If it were that simple, it would have been found already. So I find myself sitting with real patients, in the here and now, framing the illness as I have outlined here over the last year and a half. I still find the model we are evolving useful in a clinical context.
In my last practice, my interest was peak performance with respect to brain function, no matter the degree of injury or illness. I worked with the things that I found useful, personally and for my patients, most of whom had already exhausted their medical options. I was undiagnosed at that time. I knew I was sick, but it wasn’t too bad, and I knew that conventional medicine had nothing to offer me. It occurred to me now and then that I had some sort of less than MS. Other possibilities occurred as well. I tried to fit it into PTSD, but there were too many physical manifestations, hypertensive crises, arrhythmias, atypical migraines, malaise, this or that instability. I could exercise without problems for a decade. I used to say that whenever something went wrong with my body, it was undiagnosable. And I was CFIDS aware. That state of not knowing made me well suited to being a doctor of last resort. My armamentarium then was HBOT, neurofeedback, nootropics (cognitive enhancers), nutraceuticals, herbs and bioidentical hormones. I found discontinuing unnecessary drugs to be a powerful treatment modality. And I tried to create the space for the less tangible, but no less powerful healing that can happen in the context of connection and relationship.
So far, I am using pretty much the same gentle, yet powerful modalities that I used before, when I didn’t know what I was doing:), and I’m having some beginner’s luck. I am turning to these treatments first, because I know from experience, they work, and now I have a framework that gives me a better idea why. Pulsed, high dose normobaric oxygen is the most powerful and easy to deliver treatment that I have to offer. My patients so far are pretty uniformly impressed. Nobody that has rented a concentrator for a month has returned it, unless to buy one. Responses range from a little helpful to “wow”. There is a short term effect and a long-term additive effect, as I observed with HBOT in practice. It seems one of the craziest things in all this that such a simple thing has been denied us. I wonder about why, and can’t come up with much. It will never be studied, because it can’t be patented. It might accelerate aging, but the longevity folks think it’s the opposite. It needs to be more carefully dosed for patients with seizures and a few other things. Mostly, it’s probably because doctors don’t understand the gas laws, and so are uncomfortable with it. They can handle it when it comes out of a wall in a hospital, where it’s use is sanctioned, and there’s a respiratory therapist to hook things up. Otherwise, if you have COPD or are dying, you can have it. Sometimes insurance will cover it for cluster headaches, or migraines, common in our patient group. I am prescribing oxygen, for an hour a day and prn, at 10L/min by non-rebreather mask (has a reservoir and check valves), or 5-6L/min by simple mask for patients who bought lower flow concentrators (two are improving with this).
Here are a couple of references that address the oxygen paradox: Why might high dose oxygen be good for us, even though we have increased oxidative stress at baseline?
Oxidative stress, antioxidant defenses, and damage removal, repair, and replacement systems. Davies: Cells, tissues, organs, and organisms utilize multiple layers of antioxidant defenses and damage removal, and replacement or repair systems in order to cope with the remaining stress and damage that oxygen engenders. The enzymes comprising many of these protective systems are inducible under conditions of oxidative stress adaptation, in which the expression of over 40 mammalian genes is upregulated.
HIV: reactive oxygen species, enveloped viruses and hyperbaric oxygen. Baugh: ROIs repeatedly have been shown to be virucidal against enveloped-viruses, like the human immunodeficiency virus (HIV). Hyperbaric oxygen therapy (HBOT) increases the production of ROIs throughout the body, leaving no safe harbor for the virus to hide outside the genome. This technique already has been tried on acquired immune deficiency syndrome (AIDS) patients, with exciting results.
As I am finishing my first six months of practice, Ali is coming into her own, with great courage. She has enrolled for an online undergraduate program at U Mass, and will start next month. She has been dating, but still mostly staying home rather than venturing out. Right now, she is deep in the process of confronting that she is probably physically able to do more things away from home, but confined by habit and the limitations of the past. It is hugely more difficult for her than for me to emerge, without a former life to go back to.
Ali credits oxygen and modified Meyer’s cocktail infusions with her slow but continued improvement. She tells me when she feels the need for an infusion. We are still tinkering with the best formula for her. She uses oxygen 4-5 times a week, according to her own instincts. She has come to use it prophylactically for PEM, when she knows she’s overdone it. It is impossible to know what role antiretrovirals are playing in maintaining her gradual improvement which began with the cessation of Lyme treatment and was also obviously impacted by Deplin and treatment for PCOS (polycystic ovarian syndrome). Our concentrator has been broken for a couple of weeks and when the replacement came, she grabbed the mask, exclaiming “Oxygen! Mana of the Gods.” For me too, oxygen is the most tangible thing I have. It impacts my sleep directly.
 |
| click to enlarge |
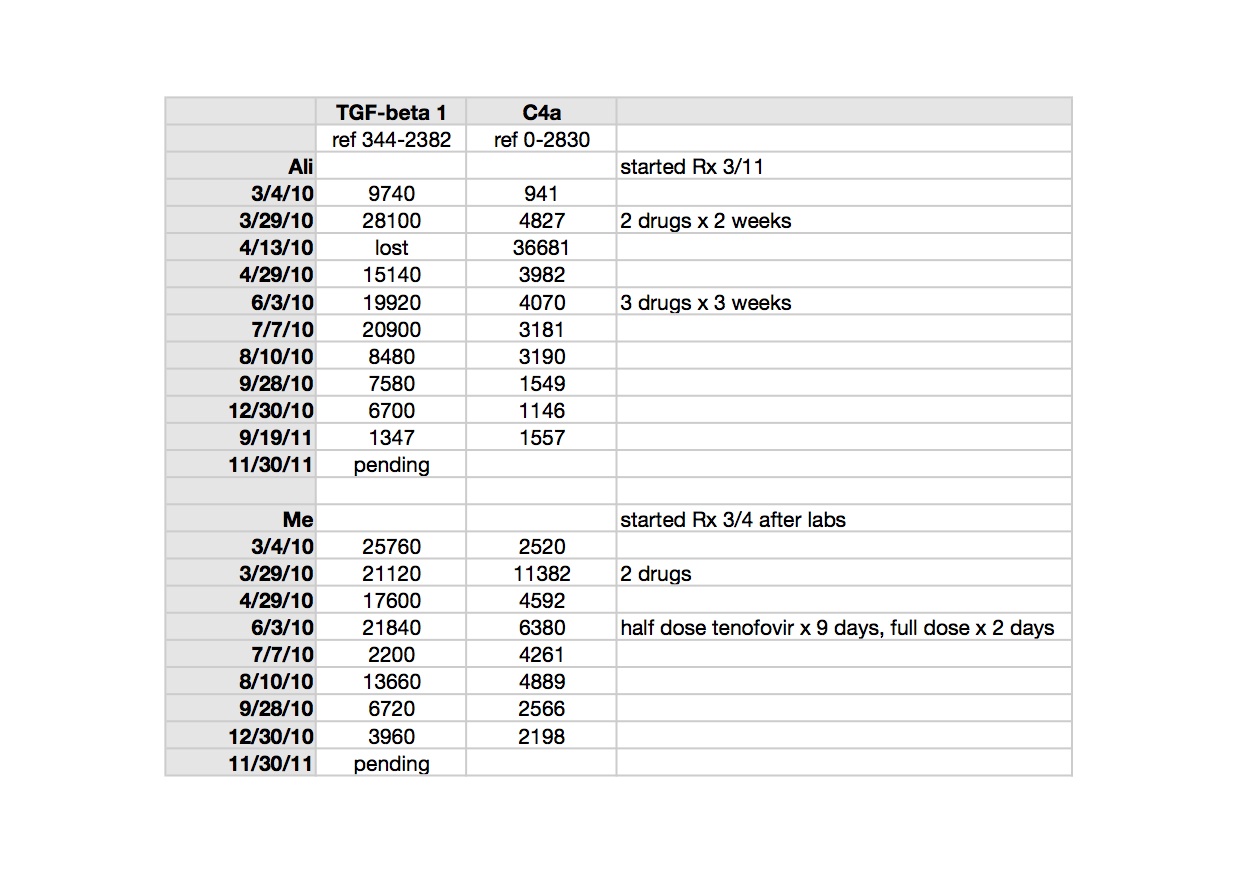
TGF beta-1 is a peptide involved in many cellular functions, including the control of cell growth, proliferation, differentiation and apoptosis. Here is a recent paper suggesting TGF beta-1 as a marker for CFS: Up-regulation of TGF-β1 mRNA expression in peripheral blood mononuclear cells of patients with chronic fatigue syndrome. Zhang. It is tempting to speculate that TGF beta-1 could be involved in the clonal expansion we are starting to think about with respect to the pathogenesis of ME/CFS and related leukemias; not forgetting that simple animal retroviruses replicate mitotically, by clonal expansion.
TGF beta-1 is implicated in the pathogenesis of Marfan’s Syndrome, which my husband’s uncle, husband and son have; in our family it appears to be more obviously expressed in each successive generation. Elevated TGF beta-1 is implicated in the pathophysiology of Marfan’s. My husband and I both had different, subclinical manifestations of illness when we met, but most, though not all, of his were attributable to Marfan’s. Marfan’s is an autosomal dominant genetic condition where chromosome 15 encodes for a defective protein which is necessary to bind TGF beta-1 to keep it sequestered to normal levels (oversimplified model). Losartan, an ARB (angiotensin receptor blocker) has been shown in clinical trials of Marfan’s patients to lower TGF beta-1 and slow the onset of the most serious consequence of the disease, aortic root dilatation. My biological father had a body habitus consistent with Marfan’s and I may be an Ehlers Danlos variant, becoming more flexible with age and exacerbations of illness. I have minor features of both conditions. Both Marfan’s and Ehlers Danlos seem to be over-expressed in the ME/CFS patient group, already showing up in my tiny practice. Here is an excellent article which considers related disorders with respect to abnormal TGF beta-1 signaling: Transforming growth factor-beta signaling in thoracic aortic aneurysm development: a paradox in pathogenesis. Jones/Ikonomidis.
>"Again, you have made up this concept in your head, but it doesn't exist in the actual reality of validation studies. This way, you can disregard any study that doesn't report the results that you want.
In actual reality, all participants can use the methodologies of their own choosing. If you read Lipkin's paper on (de-)discovery studies, you'll see that this is his modus operandi when there is enough fundig to include multiple labs."
Singh, Ruscetti, Alter, Lo, Racaniello, Mikovits have all spoken about the need to clinically validate assays. Every assays that fails to do this might as well be said to not work. So an assay that doesn't work will never detect a virus that is there. It is required by health authorities and for HIV testing you do it or end up in jail.
The methodology also includes collection and processing of samples. Mikvoits and Ruscetti wont be doing that if they are taking part in this study.
>I agree with everything that is being said here about needing to have the design published on the NIH website. I don't see any difficulty or problem with this demand.
The results are most easily explained by the fact that MRVs integrate into B cells, which tend to home in on the compartments where they first encountered the antigen, hence they would very rarely be found in blood at detectable levels.
The time is right to take the approach of tissue sampling and IHC using similar techniques that they use with HIV.
>i agree but does jamie no if mikovits has left her home and is working in a new lab with ruscetti, thats all i was wondering.
>@Anon 11:03
What are you trying to suggest with that? The study hasn't started.
>I prefer to be hopeful about Lipkin, Mikovits and Racianello. I'll wait and see what is reported.
If something comes out saying this isn't so, then it will. If not, it will come out.
Meanwhile, I'm awaiting their news.
I hope it's true that Mikovits will be working with Lipkin, etc. He did visit her at WPI and he talked to her extensively.
He spoke on viruses there and somewhere online is an 80-minute video about it, which I saw. It's not on retroviruses.
We'll just wait and see what develops.
Then you all can argue about assays and replication and validation, and where studies are posted and what you think is valid.
Meanwhile, those of us with CFS can enjoy the moment.
It is about CFS, after all, and trying to help those of us with it or future sufferers.
This isn't academic to us, but real life.
>Rachaniello is not said to be involved in the study. He has not done any research on these viruses. I think you mean Ruscetti.
The NIH website is the only way this study and the design can be announced if there are no problems with it.
>kathyd, it isn't about that at all, except for the fact that once you remove the neuroimmune disease the others are easier to study.
>It looks like part of the methodology has been conducted (Sample collection and processing) without Mikovits and Ruscetti having agreed to it.
"Lipkin had initially hoped to have the study done by the end of this year, but he now says that only about half the samples are ready to send to researchers. He plans to meet with Ruscetti and Mikovits tomorrow to hear their plans for conducting the study. “"
The study is already under way so why is the design not on the NIH website?
>Why are people being moderated on mecfsforums for pointing out that the collection/processing of those samples did not have Dr Mikovits and Dr Ruscetti's involvement?
>http://www.cfsnovel.com/blog/?p=409
>"http://www.cfsnovel.com/blog/?p=409"
Where is the NIH source for this information?
>Anon December 15, 2011 3:40 AM
"I have not seen one thing about Cheney supporting this claimed NIH study with Mikovits and Ruscetti."
Check this:
http://phoenixrising.me/archives/5778
And check a bit lower for the literal Cheney post. A snippet:
"If Judy Mikovits can, in a blinded fashion, come to the same conclusions she arrived at before in the Science paper, the sky will fall in on all other naysayers and reputations and egos will suffer great humiliation."
Luckily my reputation already stinks, but I agree that I would then suffer great humiliation (although I would suffer it with grace).
…And another snippet from Cheney:
"However, I would not want to be Switzer or the CDC or Jay Levy or Singh or John Coffin or the Science editors or most of the UK medical establishment right now.
The odds are not in their favor but we will see. I think they are all on the Titanic after what I heard today [during the Lipkin meeting]."
Seems like he is quite supportive…
Anon/V99/Tango
You are posting so much totally made up crap that it is hard to keep up. One thing that's important though:
Mikovits has been involved with the Lipkin study from the beginning and has (AFAIK) been present at every meeting. Therefore, she was consulted for the exact blood collection/storage/whatever procedures and approved all of it.
Saying that Mikovits has only now gotten involved and because some samples have already been collected shows that she had no part in this, is just patently untrue.
>@Anon December 15, 2011 3:08 PM
"Why are people being moderated on mecfsforums for pointing out that the collection/processing of those samples did not have Dr Mikovits and Dr Ruscetti's involvement?"
I wouldn't know about the moderation but what you are saying is just not true.
Mikovits was involved from the very beginning as the scientific leader of WPI. Because the study was formally conducted by WPI, Lipkin had to take some action to get Mikovits re-involved, so to say.
Because I like examples:
– Lo has been involved from the beginning as well. But suppose he would be fired at FDA tomorrow. Then, formally, the FDA would maintain to be Lipkin's "partner" for the XMRV study and Lipkin would have to take action to get Lo "re-involved". Getting him "re-involved" however, would not mean tha Lo only got involved from that point on.
>@RRM
The link you have posted if from several months ago when the Lipkin study design was different and involved different people.
If half the samples have already been collected and processed without the Mikovits/Ruscetti methodology then they are not replicating. So cannot be testing the hypothesis from Lombardi and Lo et al.
If the controls in the study are contact controls, then no one is replicating and the hypothesis from Lombardi and Lo et al. is not being tested.
Cheney has not made any comment on how he feels now with this new study. A study no one knows the design of.
"Saying that Mikovits has only now gotten involved and because some samples have already been collected shows that she had no part in this, is just patently untrue."
Are you accusing Nature of lying? Here is the quote again.
"Lipkin had initially hoped to have the study done by the end of this year, but he now says that only about half the samples are ready to send to researchers. He plans to meet with Ruscetti and Mikovits tomorrow to hear their plans for conducting the study. “"
>@RRM
"Mikovits was involved from the very beginning as the scientific leader of WPI. Because the study was formally conducted by WPI, Lipkin had to take some action to get Mikovits re-involved, so to say."
But not since the design of the study changed, as Lipkin only plans to discuss how the study is conducted with them tomorrow.
>Nope, wrong again.
There have been some problems with getting the 150 pateient samples collected. That is what he will be discussing with them tomorrow. For instance. do they want to start testing the ~75 samples now or do they want to wait until everyting is collected?
This has exactly NOTHING to do with Lipkin changing the study design without their knowledge.
That's how these things go. When something happens, you talk to the scientists involved. If tomorrow a fire destroys the collected samples, you call a meeting and see how the people involved feel, and then you make a decision on how to proceed. That is how scientist act, as I hope most ration normal people would.
But hey, keep it dark and sinister. It helps to explain everything you don't like away later on.
>@RRM
Are you accusing Nature of lying?
"Lipkin had initially hoped to have the study done by the end of this year, but he now says that only about half the samples are ready to send to researchers. He plans to meet with Ruscetti and Mikovits tomorrow to hear their plans for conducting the study. “"
Half the samples have already been collected and processed before Mikovits and Ruscetti's plans have been heard. That does not mean that there method of collecting samples or processing them is being used.
The NIH not having put this study design on their website means they are hiding something. Why? Patients are well within their rights to demand this happens immediately.
They would also be within their rights to say those samples that have been collected should not be used if they are not replicating what Mikvoits and Ruscetti would do for their clinically validated assays.
Lo's team must also state what assays they are using, or are we to take it they will use the wrong assay again from Lo et al?
The CDC should also be forced to clinically validate their assays. If they repeat any of the VP62 assays, we know they have deliberately not looked for the viruses found in Lombardi et al. as those are now proven to not be VP62.
>@RRM
"But hey, keep it dark and sinister. It helps to explain everything you don't like away later on."
Is that why they have not published the study design? Is the design totally flawed?
>Here are just three paragraphs from nature.com regarding Mikovits and Lipkin's work. This is the best news we could get at this time. We should all be celebrating. Now is not the time to snip at each other or worry about the details. That is the work of Lipkin and Mikvits, and it looks like they will get the chance to do their jobs.
http://blogs.nature.com/news/2011/12/chronic-fatigue-syndrome-scientist-finds-a-temporary-home.html#/respond
Judy Mikovits is taking her work on the road. The embattled chronic fatigue syndrome (CFS) researcher will conduct her arm of a US National Institute for Allergy and Infectious Disease (NIAID) sponsored study on the condition’s link to certain retroviruses at another US government laboratory, the scientist overseeing the study told Nature today.
W. Ian Lipkin, director of the Center for Infection & Immunity at Columbia University in New York, says that Mikovits will team up with her former mentor Frank Ruscetti at his laboratory at the US National Cancer Institute (NCI) in Frederick, Maryland. They are one of three groups testing dozens of blinded blood samples from CFS patients and healthy controls for XMRV and related retroviruses.
Lipkin came to Mikovits’ defence in her latest troubles. He says that she should be entitled to keep a copy of her laboratory records and lamented her arrest. “It’s very, very ugly and the sooner we put all this behind us the better off we’re all going to be,” he says.
"It is a fair, even-handed, noble adjustment of things, that while there is infection in disease and sorrow, there is nothing in the world so irresistibly contagious as laughter and good-humour."
– Charles Dickens, A Christmas Carol
>@Anon December 15, 2011 5:23 PM
"Half the samples have already been collected and processed before Mikovits and Ruscetti's plans have been heard."
No. Please think. I have already explained that Mikovits was involved long before this.
Tomorrow they will discuss these new developments (i.e. only obtaining half of the sapmles thus far). There have been earlier meetings where Mikovits (as well as Lo) was present.
So, no, Nature is not lying. You just have a hard time reading.
"The NIH not having put this study design on their website means they are hiding something. Why?"
You're loosing it here….
A study that's not posting its methodology on a website is "hiding something" Oh my God, Judy Mikovits has been hiding stuff her whole career, as I have never seen her posting her study design beforehand on a website.
But please keep it dark and sinister
"The CDC should also be forced to clinically validate their assays. If they repeat any of the VP62 assays, we know they have deliberately not looked for the viruses found in Lombardi et al. as those are now proven to not be VP62."
Like I have said for many months, the CDC/Sitzer will use their own assays. So no, in your world, that means they'll use "clinically unvalidated assays that are optimized for just VP62" (LOL).
But who cares? As long as Mikovits/Ruscetti or Lo can reliably discriminate between patients and controls, it's all good. Ad they should -a t least, if they were correct in the first place…
>@Anon December 15, 2011 5:27 PM
"Is that why they have not published the study design? Is the design totally flawed?"
Yes, it is. And by delaying the information until the paper's published, they'll fool the whole world!1!!1ONE!!
Except you of course…
>@RRM
"No. Please think. I have already explained that Mikovits was involved long before this.
Tomorrow they will discuss these new developments (i.e. only obtaining half of the sapmles thus far). There have been earlier meetings where Mikovits (as well as Lo) was present.
So, no, Nature is not lying. You just have a hard time reading."
The study has changed. The NIH are not putting details on their site and patients are being denied the facts. That is hiding the details.
"Like I have said for many months, the CDC/Sitzer will use their own assays. So no, in your world, that means they'll use "clinically unvalidated assays that are optimized for just VP62" (LOL)."
VP62 was not found in Lombardi et al. How can anyone justify looking for the viruses they never even detected? That is deliberately avoiding the viruses.
Clinical validation is a standard must use procedure when developing an assay. That the assay design may have changed because the samples have already gone through another procedure would mean they are not the same assays.
>"Dear Vince-
We have a plethora of explanations for how CFS/XMRV/MLV studies could go awry. However, we don’t have evidence that they have. Absent an appropriately powered study representing blinded analyses by Mikovitz and Lo/Alter of samples from well characterized subjects using their reagents, protocols and people, all we have is more confusion.
I remain agnostic. We won’t have answers until the end of 2011.
The NIH will post something on our study today.
Ian"
http://www.virology.ws/2011/05/06/ian-lipkin-on-xmrv/
Did they ever publish anything?
>"VP62 was not found in Lombardi et al. How can anyone justify looking for the viruses they never even detected? That is deliberately avoiding the viruses"
No, it is not.
Using VP62 as a control does not mean that your assay is designed to just detect that control.
For those interested, Switzer has used the Urisman/Lombardi primers, the Silverman primers, the Lo primers as well as two in-house developed primers for the pol gene.
But I guess you've already inprinted the "Switzer=VP62 searcher" idea in your mind to keep up your belief in the original results…
>@RRM
"No, it is not.
Using VP62 as a control does not mean that your assay is designed to just detect that control."
So now you admit they are not looking for the right virus. An assay optimised to VP62 uses high annealing temperatures as that is synthetic and spiked into a sample. A quote from adustymiller on mecfsforums is appropirate here.
"It is true that the PCR assays can only reliably detect viruses containing nearly exact copies of the sequences present in the PCR primers, and thus may not detect some retroviruses more distantly related to XMRV."
>@RRM
"For those interested, Switzer has used the Urisman/Lombardi primers, the Silverman primers, the Lo primers as well as two in-house developed primers for the pol gene."
Switzer has not replicated the proven clinically validated assays from Lombardi et al. Primers are only one part of an assay. Do you know what he didn't do? Or do you like misleading people?
The viruses found in Lombardi et al. have been proven to not be the prostate cancer virus called XMRV. So Urisman is irrelevant.
>"It is true that the PCR assays can only reliably detect viruses containing nearly exact copies of the sequences present in the PCR primers, and thus may not detect some retroviruses more distantly related to XMRV."
If we don't have a full sequence yet of the Lombardi et al. viruses then the labs optimising to a synthetic clone not only didn't clinically validate they didn't look for the right viruses as Lombardi et al.
As Lipkin is also in agreement that the "findings do not rule out the possibility that CFS patients are infected with related retroviruses that, for some reason, only Mikovits has been able to detect."
Well as they are proven to not be VP62 or prostate cancer viruses, then there have only been 2 studies looking for the virus. Both were positive. Both found polytropic sequences
>The fifth slide of this PowerPoint presentation totally rubbishes Coffin and Towers claims about sequence diversity being a sign of contamination. Why did they not tell people about this?
http://idrn.org/documents/events/presentations/Bangham,%20Charles.pdf
>Here is a link to an article about Drs. Lipkin, Mikovits and Ruscetti. Apparently, Drs. Mikovits and Ruscetti will be working with Dr. Lipkin at NCI labs in Maryland.
Dr. Lipkin says it is crucial that Dr. Mikovits work on this study as she found connections to retroviruses and CFS that no one else found. And that someone else at WPI isn't the same.
He says it's not right that she could not take copies of her notebooks with her.
Anyway, it looks like they will be researching other retroviruses not just XMRV.
http://www.mecfsforums.com/index.php?topic=10846.0
>@ Anon December 15, 2011 5:57 PM
"So now you admit they are not looking for the right virus. An assay optimised to VP62 uses high annealing temperatures as that is synthetic and spiked into a sample. A quote from adustymiller on mecfsforums is appropirate here."
Eh, that quote from Miller supports my position and not yours (which kames sense because you are wrong). Reasd back – he is referring to the PCR PRIMERS that determine the detection range, and NOT to the control(s) used.
@ Anon December 15, 2011 6:08 PM
"If we don't have a full sequence yet of the Lombardi et al. viruses then the labs optimising to a synthetic clone not only didn't clinically validate they didn't look for the right viruses as Lombardi et al."
Yes, they did.
Even when we totally disregard the Silverman sequences, the fact of the matter is that the remaining XMRV gag sequences show little variation and should have been picked up by those other scientists.
I understand you are emotionally clinging to the uploaded env sequences that are not identical to XMRV, but the problem is that Lombardi et al. searched for gag sequences. Looking at the gag sequences they found and uploaded to Genbank, other scientists should have had no problem finding them as well – sequences variation could really have not been an issue with regard to the used gag primers, based on all the gag sequences reported by the Mikovits lab.
"As Lipkin is also in agreement that the "findings do not rule out the possibility that CFS patients are infected with related retroviruses that, for some reason, only Mikovits has been able to detect." "
Of course, because it's true. It is true for almost every claim. That is why you put the person who makes such a claim to the (independently blinded) test. Mikovits failed to discriminate between self-designated positives and negatives earlier, and now we'll see if she'll be able to disciminate between patients and controls.
Based on what I know of the situation, I find it very unlikely that she will succeed, but I'll be happy to be proven wrong. It seems to me that you don't have much confidence in her either – why would you already be making up all kinds of excuses?
>@Kathy
An assay that is optimised to VP62 cannot be looking for other MRVs as the PCR conditions are incorrect and the assay would only be able to detect that strain, which has never been found in nature. The CDC use only such assays
>@Kathy D
"[Lipkin] says it's not right that she could not take copies of her notebooks with her."
Problem is that there is no evidence that she did ask for (and was denied acces to) copies. After Mikovits got fired, she gained EXCLUSIVE control of those notebooks. Thus, it seems that it was not just about getting "copies".
As Mikovits's lawyer Scott Freeman explained, "explaining to a scientist how the criminal system works is like a scientist explaining to us how to cure cancer".
I guess this applies to Ian Lipkin as well. .. ;-)
>@RRM
It is still over your head and beyond your education.
VP62 has nothing to do with the Lombardi findings. Primers set to areas not sequenced by Lombardi et al but to regioms of man made VP62 cannot therefore be targeted at the Lombardi viruses.
PCR optimised to a free floating synthetic virus is inappropriate for detecting an integrated virus in an highly methylated state. You cannot claim anything would have been found as the few assays looking for gag are unproven. Most studies did not look for gag and all change their PCR variables. The conditions described will require very specific PCR variables. Hanson confirmed a 1 degree change annealing temp was enough to render the virus invisible to her assay.
Analytical validation provides no data on clinical validation
which must be provided to ensure an assay can detect the viruses present. This is why it is illegal test a person for HIV with an assay not clinically validated. What are you afraid they will be optimising to?
When ever Mikovits has tested blinded samples the results are always consistent with the findings of Lombardi et al. Mikovits did not do the BWG study that was a mess of a paper with assay alterations none replication only looking for vp62 controls not included. If this had been used on HIV the human race would now be in a very sorry state.
So what do you think the labs with unproven assays are optimising to when they use a clinical positive? if the labs claim they can control contamination what are you concerned they will design an assay to detect?
>@RRM
You have always been very uncomfortable knowing the police are tracing you about the Lombardi raw gel you were posting on the web.
You can continue to make up stories, but how can Mikovits have had exclusive control when she didn't posses them, but you and Billy were posting that gel?
Mikovits also had a legal obligation to protect the Lombardi data that was now being posted on the web and we don't know when or if she ever took anything at any time after Max claims he left her with some notebooks
We also don't know who owns the materials. As all Lombardi methods are in the public domain anyway, no one can be accussed of trying to take those materials either.
Would you like to now tell everyone the truth about the source of the gel?
>I'll give Dr. Mikovits and Dr. Lipkin the benefit of the doubt, as I have sympathy for a scientist and her data, and another researcher who understands her attachment to her work — and the possible help it could offer for their studies.
We'll see what happens, but I am not condemning either person here.
This blog isn't a court. It's a blog to understand and discuss CFS. Most of have it.
We're going back to this criticism again, just when it came out that she and Dr. Ruscetti will work at NCI with Dr. Lipkin.
I'm not going to do that. We, those of us with CFS, want to see what develops and have hope. It's the first hopeful sign in all of this uproar.
Let's not throw the baby out with the bath water here. Wow, am I dating myself with that one.
Anyway, a good development happened. I want to see what happens. There's hope around the CFS part of the blogosphere again. That's important.
Let's not act like judges, let's act like people who want to help.
>Now we need the NIH to publish the full design of the study on their website in the interests of transparency. That should be not an issue if they are hiding nothing. We do not want a repeat of the messed up blood study.
That will then ensure Mikovits and Ruscetti can replicate their clinically validated assays. To do this would also require those samples so far taken be discarded if they have not been collected and processes according to the clinically validated assay designs.
>@Anon December 16, 2011 2:14 AM
It's a bit too much fo my education really, so I will just quote this gem:
"This is why it is illegal test a person for HIV with an assay not clinically validated."
Problem is that, unlike XMRV, with HIV we are not in the validation stage.
AFTER a finding is validated and people AGREE on positive findings, it is normal and accepted practise to check any newely developed assay against these positive findings.
When people are still arguing whether someone's positive findings are really positive findings (i.e. during the validation stage itself) then it is dumb to use one of the known positives (according to one group) as validation for the methodology of the other group.
I am sure you have already made up your mind, but for the lurkers:
– Suppose I am producing a new telescope to look at the moon's craters. As we all agree that the moon has many craters and there are also multiple lines of evidence on the location of many craters, it is perfectly fine for me to "clinically valaidate" my telescope through "known positive" craters.
However, suppose I have this new telescope and I think it can detect craters on the surface of the sun. Other scientists think I am crazy because they can't reproduce my findings using their telescopes. In this "validation stage" context, I hope it is perfectly clear that it is unaceptable that these other scientists should show that their telescopes work through detection of my "known positive" craters.
In the second scenario, we are actually trying to agree on whether my findings are true or not. Incorporating the assumption that I am correct in the experiments of others, would lead to dependent and circular experiments by others instead of independent validation.
@ Anon December 16, 2011 2:23 AM
"You have always been very uncomfortable knowing the police are tracing you about the Lombardi raw gel you were posting on the web."
Oh no, not this again. Have you not read JDJ's request to stop posting about this?
In any case, if the US cops are truly chasing me, they truly suck balls because it would be very easy to do so.
They don't however, because *they* are not crazy.
>@RRM
The findings are already validated by multiple labs, methods, and use of clinically validated assays. Basics RRM, learn them first.
Without clinical validation an assay is unproven. These assays therefore do not work and cannot detect a positive. LOL "we are not in the validation stage" you say. Then how can people be told they are negative? Patients are not falling for it.
Let's be sensible, a telescope to look at the moon will be altered to look at the sun. It will have to be optimised to the sun and if that fails as a scientist you ae obligeged to then use the proven method. So the same telescope design. from the same location as this is a telescope. This is what you fail to understand. There are also multiple lines of evidence that shows the viruses are infecting people.
You avoided this question. so lets try again. What do you think they are optimising to when a scientists clinically validates an assay using a positive?
>@RRM
You were posting a raw gel when material was said to have been stolen. Don't think anyone would fall for " the police are not crazy enough to trace me". It also won't only be the police.
>@ Anon December 16, 2011 3:37 AM
"The findings are already validated by multiple labs, methods, and use of clinically validated assays. Basics RRM, learn them first."
If we are already "out" of the validating process, then why are we still having all those validation studies?
As long as there is no agreement on the data, assuming the data are correct for the purpose of another study is stupid.
But keep repeating the meme. Like I said, because nobody will actually employ your (stupid) methodology, you can baisically ignore any future result that you don't like.
"You were posting a raw gel when material was said to have been stolen. Don't think anyone would fall for " the police are not crazy enough to trace me". It also won't only be the police."
Oh, I am now so nervous about this. They're all chasing me. Who are the others? The department of stupid?
But Please keep repeating it in your head. I don't even want to guess if you are sick enough to believe it all or are just blatently lying to draw attention away from the real culprits.
>@RRM
"If we are already "out" of the validating process, then why are we still having all those validation studies?"
Yes why are we! This should have been allowed to move onto clinical trials, instead of having it slowed down and blocked by people with vested interests and politics.
"As long as there is no agreement on the data, assuming the data are correct for the purpose of another study is stupid."
There is no such thing as consensus science.
"But keep repeating the meme. Like I said, because nobody will actually employ your (stupid) methodology, you can baisically ignore any future result that you don't like."
Who's methodology?
"Oh, I am now so nervous about this. They're all chasing me. Who are the others? The department of stupid?
But Please keep repeating it in your head. I don't even want to guess if you are sick enough to believe it all or are just blatently lying to draw attention away from the real culprits."
Welcome to the real world RRM.
>December 16, 2011 5:19 AM
"Yes why are we! This should have been allowed to move onto clinical trials, instead of having it slowed down and blocked by people with vested interests and politics."
Okay. You don't believe the Singh, Levy, BWG and Lipkin studies to be validation studies because we were already out of the validation process?
I am the one living in a fairy tale world, right…
"There is no such thing as consensus science."
It has little to do with consensus science. Scientists rely on previous, undisputed data to be correct. That's the whole idea of the scientific method: to build on pervious knowledge.
If tomorrow a theory thought to be correct turns out to be incorrect after all, then all the experiments that relied on that theory being true basically go down with it.
This is exactly why validation studies cannot rely on the original study. You could still do some follow-up experiments on the basis that your original experiment may be true, but one cannot rely on the original study when one is trying to independently validate it.
It has never happened and it never will, and *validation* of HIV assays has nothing to do with the independent *validation* attempts of Lombardi (and Lo) et al.
"Welcome to the real world RRM."
But in that *real* world, I have yet to hear from the police or from the other people that are chasing me in your fairy tale world…
..where waters gushed and fruit trees grew,
and flowers put forth a fairer hue,
and everything was strange and new…
>"Okay. You don't believe the Singh, Levy, BWG and Lipkin studies to be validation studies because we were already out of the validation process?
I am the one living in a fairy tale world, right…"
None of them used clinically validated assays. Assays not proven.
"It has little to do with consensus science. Scientists rely on previous, undisputed data to be correct. That's the whole idea of the scientific method: to build on pervious knowledge.
If tomorrow a theory thought to be correct turns out to be incorrect after all, then all the experiments that relied on that theory being true basically go down with it. This is exactly why validation studies cannot rely on the original study. You could still do some follow-up experiments on the basis that your original experiment may be true, but one cannot rely on the original study when one is trying to independently validate it. It has never happened and it never will, and *validation* of HIV assays has nothing to do with the independent *validation* attempts of Lombardi (and Lo) et al."
There is no such thing as undisputed data RRM. There are only probabilities. Yes people should build. Looking for the wrong viruses and not clinically validating is not building. Lombardi and Lo et al made the same findings, there sequences are both polytropic.
"But in that *real* world, I have yet to hear from the police or from the other people that are chasing me in your fairy tale world…"
I have never known such a case to move that fast. Is there any topic you have any modicum of knowledge of?
>"None of them used clinically validated assays. Assays not proven."
You are contradicting yourself. Either you argue that:
a) these studies are not validation studies because the validation process is already far behind us. Therefore assays dhould be validated.
or
b) you accept that these are validation studies in which there is no place for validation to results you are trying to independently validate.
However, you argue at the same time that these are validation studies that should validate their assays to to results of the study that they're trying to validate, AND that the validation process is already far behind us.
"There is no such thing as undisputed data RRM. There are only probabilities. Yes people should build. Looking for the wrong viruses and not clinically validating is not building. Lombardi and Lo et al made the same findings, there sequences are both polytropic."
Keep drinking that cool-aid.
Yes, nothing is absoluetly "undisputed". That is why I explained that "undisputed" results can turn out to be incorrect after all in my post you are replying to.
You assume I lack the necessary knowledge in some areas, but you lack the necessary reading comprhension skills to even seriously argue about anything.
"I have never known such a case to move that fast. Is there any topic you have any modicum of knowledge of?"
This just proves that you don't know much. Cases do move that fast. Remember how fast an independent judge granted search warrants for Mikovits's and Meehan's homes? Should be easy to obtain permission to check some IP addresses (where privacy rights are far less in play than with searches of peoples' homes)
>@RRM
Again it is over your head
"a) these studies are not validation studies because the validation process is already far behind us. Therefore assays dhould be validated.
or
b) you accept that these are validation studies in which there is no place for validation to results you are trying to independently validate."
The validation process is over after multiple assays and studies, they can use clinically validated assay on the known positives, but failed to do so rendering their results useless.
"Yes, nothing is absoluetly "undisputed". That is why I explained that "undisputed" results can turn out to be incorrect after all in my post you are replying to."
There are only probabilities. No evidence exists to show any positive paper is wrong.
"You assume I lack the necessary knowledge in some areas, but you lack the necessary reading comprhension skills to even seriously argue about anything."
You prove my point and provide no argument.
"This just proves that you don't know much. Cases do move that fast. Remember how fast an independent judge granted search warrants for Mikovits's and Meehan's homes? Should be easy to obtain permission to check some IP addresses (where privacy rights are far less in play than with searches of peoples' homes)"
They can have already have checked IP addresses. Now they will be checking out other IP address also. You build the case and then question suspects. The incident you highlight was outside of what had been implemented, but a judge can take emergency measures to protect items if they are told this needs to happen. Whether the judge in this case should have order such a thing will be part of the case.
>@RRM
You keep avoiding the question. What do you think they are optimising to when they use a known positive?
>@Anon December 16, 2011 8:48 AM
"You prove my point and provide no argument."
I am glad you then agree with my initial post. Remember, you argued againts my post by saying something ("science is not indisputed") that was no contradicting my post when read in its proper context.
"You keep avoiding the question. What do you think they are optimising to when they use a known positive?"
Another fatal answer. Now, for the sake of your argument:
optimising = calibrating?
Yes, it must be me. Not you…
>@RRM
You are still avoiding the question. What do you think they are optimising to when they use a known positive?
>In Vitro is not a psychiatrist, or if so it is secondary nature. My bet is he/she is an neurodiverse saddo who has bought into the religion of autism being genetic, set in stone and untreatable, someone who has staked all of his/her self-esteem on this myth. Pathological findings in autism will be denied to death, and so will any environmental (preventable and treatable) causative factors, for those threaten to blow down his/her house of cards.
>@Anon 9:32
InVitro has also not denied they are a member of the Wessely School or BACME.