
One morning an elderly man was walking on a nearly deserted beach after a big storm had washed up thousands and thousands of starfish. He came upon a boy who was picking them up and throwing them back into the ocean, as eagerly as he could.
Puzzled, the older man looked at the young boy and asked, “Little boy, what are you doing?”
The youth responded without looking up, “I’m trying to save these starfish, sir.”
The old man chuckled aloud, and queried, “Son, there are thousands of starfish and only one of you. What difference can you make?”
Holding a starfish in his hand, the boy turned to the man and, gently tossing it into the water, said, “It will make a difference to that one!”
It is all well and good to say that now that XMRV is dead, science can get back to its orderly, stepwise process; they even get to say, we told you so. And I say what I have said all along: millions of patients need treatment now. It is not a static situation. It is a progressive disease, slow, but lots of people are circling the drain. Many new cases that might be easier to treat sooner rather than later… that might respond more completely to arv’s. New babies being born with it. Should we wait a decade to start to find out, in a systematic way, if existing treatments might not affect it? It is incumbent upon the medical and pharmaceutical industries to think about the disease in concept and find solutions, not sit there doing nothing until Virus X is found; that approach already hasn’t worked for decades. It is quite likely that it won’t turn out to be a one virus, one disease, one treatment paradigm. If it were that simple, it would have been found already. So I find myself sitting with real patients, in the here and now, framing the illness as I have outlined here over the last year and a half. I still find the model we are evolving useful in a clinical context.
In my last practice, my interest was peak performance with respect to brain function, no matter the degree of injury or illness. I worked with the things that I found useful, personally and for my patients, most of whom had already exhausted their medical options. I was undiagnosed at that time. I knew I was sick, but it wasn’t too bad, and I knew that conventional medicine had nothing to offer me. It occurred to me now and then that I had some sort of less than MS. Other possibilities occurred as well. I tried to fit it into PTSD, but there were too many physical manifestations, hypertensive crises, arrhythmias, atypical migraines, malaise, this or that instability. I could exercise without problems for a decade. I used to say that whenever something went wrong with my body, it was undiagnosable. And I was CFIDS aware. That state of not knowing made me well suited to being a doctor of last resort. My armamentarium then was HBOT, neurofeedback, nootropics (cognitive enhancers), nutraceuticals, herbs and bioidentical hormones. I found discontinuing unnecessary drugs to be a powerful treatment modality. And I tried to create the space for the less tangible, but no less powerful healing that can happen in the context of connection and relationship.
So far, I am using pretty much the same gentle, yet powerful modalities that I used before, when I didn’t know what I was doing:), and I’m having some beginner’s luck. I am turning to these treatments first, because I know from experience, they work, and now I have a framework that gives me a better idea why. Pulsed, high dose normobaric oxygen is the most powerful and easy to deliver treatment that I have to offer. My patients so far are pretty uniformly impressed. Nobody that has rented a concentrator for a month has returned it, unless to buy one. Responses range from a little helpful to “wow”. There is a short term effect and a long-term additive effect, as I observed with HBOT in practice. It seems one of the craziest things in all this that such a simple thing has been denied us. I wonder about why, and can’t come up with much. It will never be studied, because it can’t be patented. It might accelerate aging, but the longevity folks think it’s the opposite. It needs to be more carefully dosed for patients with seizures and a few other things. Mostly, it’s probably because doctors don’t understand the gas laws, and so are uncomfortable with it. They can handle it when it comes out of a wall in a hospital, where it’s use is sanctioned, and there’s a respiratory therapist to hook things up. Otherwise, if you have COPD or are dying, you can have it. Sometimes insurance will cover it for cluster headaches, or migraines, common in our patient group. I am prescribing oxygen, for an hour a day and prn, at 10L/min by non-rebreather mask (has a reservoir and check valves), or 5-6L/min by simple mask for patients who bought lower flow concentrators (two are improving with this).
Here are a couple of references that address the oxygen paradox: Why might high dose oxygen be good for us, even though we have increased oxidative stress at baseline?
Oxidative stress, antioxidant defenses, and damage removal, repair, and replacement systems. Davies: Cells, tissues, organs, and organisms utilize multiple layers of antioxidant defenses and damage removal, and replacement or repair systems in order to cope with the remaining stress and damage that oxygen engenders. The enzymes comprising many of these protective systems are inducible under conditions of oxidative stress adaptation, in which the expression of over 40 mammalian genes is upregulated.
HIV: reactive oxygen species, enveloped viruses and hyperbaric oxygen. Baugh: ROIs repeatedly have been shown to be virucidal against enveloped-viruses, like the human immunodeficiency virus (HIV). Hyperbaric oxygen therapy (HBOT) increases the production of ROIs throughout the body, leaving no safe harbor for the virus to hide outside the genome. This technique already has been tried on acquired immune deficiency syndrome (AIDS) patients, with exciting results.
As I am finishing my first six months of practice, Ali is coming into her own, with great courage. She has enrolled for an online undergraduate program at U Mass, and will start next month. She has been dating, but still mostly staying home rather than venturing out. Right now, she is deep in the process of confronting that she is probably physically able to do more things away from home, but confined by habit and the limitations of the past. It is hugely more difficult for her than for me to emerge, without a former life to go back to.
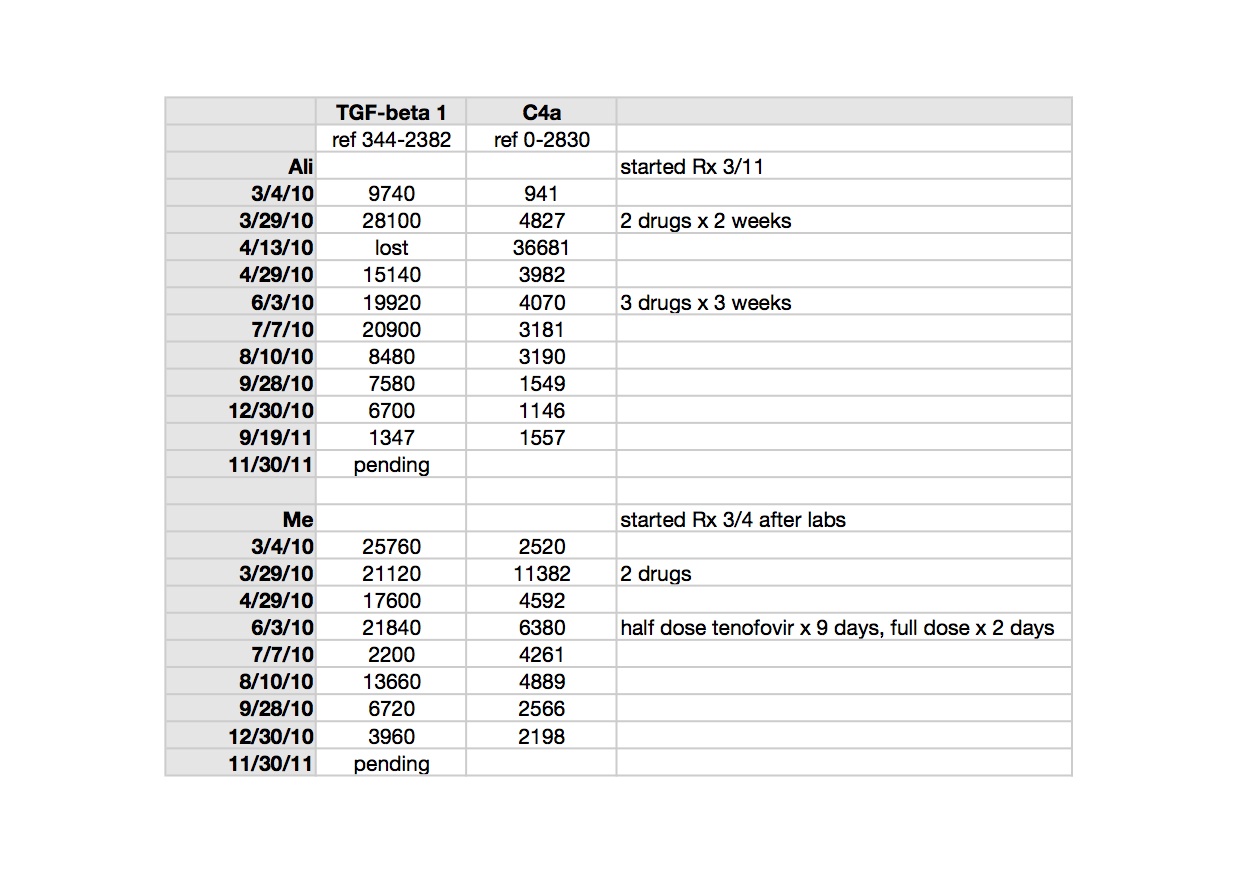
Ali credits oxygen and modified Meyer’s cocktail infusions with her slow but continued improvement. She tells me when she feels the need for an infusion. We are still tinkering with the best formula for her. She uses oxygen 4-5 times a week, according to her own instincts. She has come to use it prophylactically for PEM, when she knows she’s overdone it. It is impossible to know what role antiretrovirals are playing in maintaining her gradual improvement which began with the cessation of Lyme treatment and was also obviously impacted by Deplin and treatment for PCOS (polycystic ovarian syndrome). Our concentrator has been broken for a couple of weeks and when the replacement came, she grabbed the mask, exclaiming “Oxygen! Mana of the Gods.” For me too, oxygen is the most tangible thing I have. It impacts my sleep directly.
 |
| click to enlarge |
TGF beta-1 is a peptide involved in many cellular functions, including the control of cell growth, proliferation, differentiation and apoptosis. Here is a recent paper suggesting TGF beta-1 as a marker for CFS: Up-regulation of TGF-β1 mRNA expression in peripheral blood mononuclear cells of patients with chronic fatigue syndrome. Zhang. It is tempting to speculate that TGF beta-1 could be involved in the clonal expansion we are starting to think about with respect to the pathogenesis of ME/CFS and related leukemias; not forgetting that simple animal retroviruses replicate mitotically, by clonal expansion.
TGF beta-1 is implicated in the pathogenesis of Marfan’s Syndrome, which my husband’s uncle, husband and son have; in our family it appears to be more obviously expressed in each successive generation. Elevated TGF beta-1 is implicated in the pathophysiology of Marfan’s. My husband and I both had different, subclinical manifestations of illness when we met, but most, though not all, of his were attributable to Marfan’s. Marfan’s is an autosomal dominant genetic condition where chromosome 15 encodes for a defective protein which is necessary to bind TGF beta-1 to keep it sequestered to normal levels (oversimplified model). Losartan, an ARB (angiotensin receptor blocker) has been shown in clinical trials of Marfan’s patients to lower TGF beta-1 and slow the onset of the most serious consequence of the disease, aortic root dilatation. My biological father had a body habitus consistent with Marfan’s and I may be an Ehlers Danlos variant, becoming more flexible with age and exacerbations of illness. I have minor features of both conditions. Both Marfan’s and Ehlers Danlos seem to be over-expressed in the ME/CFS patient group, already showing up in my tiny practice. Here is an excellent article which considers related disorders with respect to abnormal TGF beta-1 signaling: Transforming growth factor-beta signaling in thoracic aortic aneurysm development: a paradox in pathogenesis. Jones/Ikonomidis.
>"Our informal survey shows us that the incidence of ASD in offspring and siblings of CFS women is much higher than in the general population."
But that's the problem with 'informal [health] surveys', there's a huge participatory confirmation bias where those who have a feature to report participate, and those who do not, abstain. All your survey has told you is that certain people are more likely to contribute to it than others. That's not epidemiology, and making any projection from it is absent of any scientific validity. Even if the survey was somehow representative there would still be no basis to deduce causal relationship without excluding numerous confounding factors. And even were the confounding factors to be addressed any causal relationship could be the reverse of what you imply – for instance it could be that having an ASD child is more likely to evoke symptoms of chronic fatigue in mothers.
>"… symptoms of chronic fatigue in mothers."
So, In Vitro, what is the reason you keep reading this blog?
What is your connection to the topic of this blog?
Do you have a connection to the topic of this blog?
>Is it your opinion that we are discussing THAT?
Do you think Jamie's survey is about THAT?
Well, do you?
>"But that's the problem with 'informal [health] surveys', there's a huge participatory confirmation bias where those who have a feature to report participate, and those who do not, abstain"
That is every paper from the Wessely school and CDC that you have described.
They want to pretend rates are not increasing and there is no link. To ensure this they do no studies of their own using ME criteria. No data is held on rates, associations and deaths. That is the trouble with working for the money and not acting like a scientist.
>In Vitrio you say these studies don't exist, but you state you know the answer already. Your beliefs are irrelevant.
>@In Vitro, you are absolutely right of course, but save your breath because the majority here does not seem interested in facts, other than those they "know" to be true regardless of what the data all say.
>What is it that YOU "know" to be true?
>well I am sick, but would I give babies arv's ?
I really don't know, I know I really wouldn't want to.
In ref to mothers having cfs as a result of having a child with autism, well yes, if cfs is a cohort of Tired All The Time CDC/Wessley fav patient picks.
But ME surely is different!
Age of Autism's Ken seems very knowledgeable about Autism, and he is extremely concerned about XMRVs involvement in Autism.
@Anon from December 13, 2011 8:54 AM
I do hope you will never have to contemplate that reality personally, but if you do, I hope yr words bite.
>"@In Vitro, you are absolutely right of course, but save your breath because the majority here does not seem interested in facts, other than those they "know" to be true regardless of what the data all say."
You and In Vitro are the type who don't want to test any hypothesis that threatens your mind set.
>In Vitro which member or the Wessley school or BACME are you?
>In Vitro et al,
All surveys have to overcome the issue of selection bias, and all epidemiological studies are flawed in some way, which doesn't render them useless. That's why we are planning to redo it properly with a control group. I'll grant you that our survey might have preselected for people with sick family members, though we got lots of negatives too. But our first pass look at what we got says that if you have CFS, your chance of having an autistic child is increased by many times what CDC data predicts. Our informal survey taught us what questions to ask. We know we need a control group.
Still if I could show you that 1000 offspring of a few hundred people with CFS included 50 or 75 autistic children, instead of the expected 10, would that say anything to you?
Why are you so sure that our data is invalid? What's your stake in believing it wrong? If anyone has ideas about how to structure a study that In Vitro would believe, I'm all ears…
Jamie
>In Vitro, is your real problem with In Vivo?
>why is no one talking about the roche germany people who say they found xmrv by next generation sequencing?
>Probably this
"”There is increasing concern that in modern research, false findings may be the majority or even the vast majority of published research claims…Conflicts of interest are very common in biomedical research, and typically they are inadequately and sparsely reported…Prestigious investigators may suppress via the peer review process the appearance and dissemination of findings that refute their findings, thus condemning their field to perpetuate false dogma. Empirical evidence on expert opinion shows that it is extremely unreliable…Highly prejudiced stakeholders may even create a barrier that aborts efforts at obtaining and disseminating opposing results…”
Ioannidis JP. Why most published research findings are false. PLoS Med. 2005 Aug; 2(8): e124. http://medicine.plosjournals.org/perlserv/?request=get-pdf&file=10.1371_journal.pmed.0020124-L.pdf
— John P.A. Ioannidis, MD, Dept. of Hygiene and Epidemiology, University of Ioannina School of Medicine, Greece; Institute for Clinical Research and Health Policy Studies, Dept. of Medicine, Tufts-New England Medical Center, Boston
>In vito infidelium,
I can't speak to autism relevant to CFS but there was an epidemiological study done by Lenny Jason, PhD in Wichita, KS. Turns out there were quite a few family members, not blood relatives who were also sick with CFS. Now this could have been because the home had carbon monoxide, toxic mold, who knows. It could have been that the cause is some mildly contagious but severe pathogen. There were more cases in rural areas. Also, there were plenty of cases in African Americans and poor country folks, not just white yuppies. So this still leaves many questions, but at least some direction to head and infection is certainly one direction, also how female hormones might influence susceptibility.
Paula – a white, female ex-yuppie too sick to yup anymore
Retrovirolist,
Don't be intimidated by the confrontationalists on this list. I am a kind, polite ex-yuppie and would love to hear your thoughts on my posts. Not that I will always agree, but at least I will respect your right to think and use your expertise to sort through all the crap, uh, feces (a more scientific term).
>Not to steal your topic at all, but in the same "why" genre:
Why are retrovirologists not talking about this AIDS-like disease and how they can search vigorously for a retrovirus?
"XMRV is a contaminant" is not a cogent argument against the plausibility of a retrovirus.
How about getting in the lab and looking for signs of retroviruses using ICC?
Why aren't they talking about how they can save lives?
Why are they blase?
>@Paula
"Not that I will always agree, but at least I will respect your right to think and use your expertise"
Why do you even think they are a retrovirologist? That haven't given any proof of this and we see virologists all the time doing all they can to not find anything.
>"why is no one talking about the roche germany people who say they found xmrv by next generation sequencing?"
John Coffin the man with the funny idea about a special event creating a retrovirus in cells that would never happen but did. Lol Did publish two papers this last year that found the viruses in prostate cancer and HIV patients. He had no explanation for detecting those viruses in those patients at 12% and 2% respectively.
The immaculate contamination brigade don't like talking about that either.
>Why would anyone who calls him/herself a retrovirologist or a virologist have a vested interest in denying a cause to CFS? What is in it for you?
Have you no concern or compassion for people who are sick every single day of their lives, whose every move is determined by their disease, who have to worry every moment about what will exacerbate their symptoms?
There is a lot of arrogance here among people who are in an ivory tower or think they are, blithely discussing a disease which is ravaging tens of thousands of people, more actually. Or should I say dismissing, rather than discussing?
You all should be championing research, pushing for it, demanding it.
If you aren't part of the solution, you are part of the problem. Really!
I don't think any of us need more nay-sayers. We really don't.
We need people to think and try to help figure this out, not to harass us with their repeated posts on the same things which are of no help.
We need thinking, creativity, hard work, not negativity and dismissal of our disease or our comments. We live with this disease.
Does anyone who doesn't have CFS get it at all?
I find among my friends that health professionals understand the least. They go by antiquated textbooks and can't see the living person in front of them with symptoms.
I really wish the cause and treatment would be found for all of our sakes. And the nay-saying and negativity would stop. If there is nothing productive and helpful to say, don't say anything.
>JDJ December 13, 2011 11:58 AM: “Why are you so sure that our data is invalid? What's your stake in believing it wrong? If anyone has ideas about how to structure a study that In Vitro would believe, I'm all ears…”
There is no single study that I would ‘believe’; multiple studies of variant methodology defining commonly supportable observation, would however encourage me to weight probability on those observations as describing a real phenomenon. I have no idea – and neither have you, whether or not your data is valid because you have no way of validating it. The survey model is profoundly limited in its usefulness in health science settings and I no more accept the findings of Reeves et al in their use of it than I do yours. Anything that is dependent upon ‘patient’ report is highly suspect when used to extrapolate epidemiologically.
If the hypothesis under test is “ Women with CFS (nullipara or post partum or both ?) have an unexplained preponderance to have children who develop ASD”, then the only valid methodologies are those where independent authority is responsible for confirmation of mother’s diagnostic status and separately ‘child’s diagnostic status. To have epidemiological relevance the research population would have to be of a size which allows exclusion of the probabilistic occurrence of random statistical artefacts – given the percentage occurrence of both ASD and CFS in the general population, the research scope would need to be in thousands or higher. The ideal data sets therefore would be those produced by public health monitoring bodies. There are numerous proposed prenatal factors for ASD prevalence, see: http://bjp.rcpsych.org/content/195/1/7 one of the many challenges for the CFS/ASD hypothesis is to be able to distinguish between CFS as a causal link and any of the other proposed multiple predispositions. It’s not difficult to see the likely problems for example that age profiles might cause, if mother’s age is indeed indicative of prevalence of ASD, and diagnosis of CFS is heavily weighted to women over the age of 35, then there is a definitive confounding factor which can only be excluded (assuming that exclusion is even possible) by having a sufficiently powered (i.e large) study. An ‘opt in’ survey comes no where near addressing these types of problem and only serves to tell those involved a story that has no scientific validity what so ever. Of course if there are M.E/CFS affected people who want to go down the AoA route of crank medicine, then they are obviously free to do so, but not everyone with M.E/CFS wants to be part of that kind of bunker asylum.
>"There is no single study that I would ‘believe’; multiple studies of variant methodology defining commonly supportable observation, would however encourage me to weight probability on those observations as describing a real phenomenon. I have no idea – and neither have you", whether or not your data is valid because you have no way of validating it.
Multiple studies using strict ME criteria would provide answers. That is why health bodies domt fund them. Replication is still a fundamental of the scientific method. stop pretending it isn't.
Which member of the Wessely school are you and how long have you been a psychiatrist?
>"if mother’s age is indeed indicative of prevalence of ASD, and diagnosis of CFS is heavily weighted to women over the age of 35, then there is a definitive confounding factor which can only be excluded"
That is fatigue not ME. Let's stick to what is proveable from using science.
>odd box question.
Is there any risk to a foetus if it is exposed to chicken pox?
ie my eldest child having chicken pox when I was pregnant with my second child.
or my eldest child being vaccinated against chicken pox while i am pregnant with my second child?
>Is there any new news about Dr. Mikovits? About XMRV now that Roche has found the virus?
Why are we being kept in the dark when we are dying???
>Yes, In Vitro, we are aware that our controls need to be age matched. And that someone like you would need multiple studies with variant methodologies. Me too. But at this point there are none at all and someone needs to do the first one. Pretty clearly it isn't going to be the people who are being paid to protect the public's health. They will have to explain the extended coffee breaks they took while the health of the species was destroyed.
And how would you explain these 3 findings in one study?
1. People with the symptoms of ME/CFS have a much increased risk of their children and siblings being autistic, many times predicted.
2. People with the symptoms of ME/CFS have a much increased risk of their children having CFS, many times predicted.
3. Partners of people with the symptoms of ME/CFS have a much increased risk of developing CFS, many times predicted.
In addition, but it will require a very large study to show statistical significance, certain genetic diseases, autoimmune diseases, neurodegenerative diseases and cancers, especially leukemias, are over-represented in the patient group and immediate family members. I predict that PCOS, Hashimoto's thyroiditis and possibly Marfan's Syndrome will reach significance in the patient group.
I challenge any epidemiologists reading to join us, or do the study yourself. It's a really good study. Earthshaking.
Why are you so invested in it not being an infectious disease? I am assuming that you are a man, but men hide that they are ill. Do you have it? Are you working in the lion's den, trying not to be eaten?
Jamie (experiment in vivo)
>I forgot health care workers. I think it will turn out that ME/CFS is overrepresented in health care workers, including veterinarians.
Jamie
>"They will have to explain the extended coffee breaks they took while the health of the species was destroyed."
Deal with it people! We will help those who face up to the truth. We cannot afford to ignore this and leave people to die in pain.
>Patients who submitted surveys had already been seen by physicians, usually ME/CFS specialists. The diagnosis of ME/CFS is not in the mainstream lexicon and I believe it unlikely that a patient would assume this label without consulting physicians, especially as it puts them in an unfavorable position to receive adequate medical care. It is not realistic to say that a child's diagnosis of ASD would be imagined by the mother, this diagnosis is serious and as treatment is often attempted, has to be validated by a physician. Third party payers require a physician's input for allowing treatments for ASD.
An issue is made as to age of the mother and this is appreciated, however it should be easy to get age matched controls. Any further constructive suggestions would be appreciated. Phrases such as "crank medicine" and "bunker asylum" are neither scientific nor constructive.
Another point made was lack of supervision. All the results are reviewed by physicians and clarified by direct communication with the patients. This goes beyond the usual check list epidemiologic study that is published and as we know epidemiologic studies are published almost weekly in journals such as NEJM and JAMA.
Finally the purpose of this survey is to raise interest for further research in ME/CFS. No treatment recommendations are being made but we do hope that research will include testing of all reasonable options of therapy. We also hope that scientists will remain objective; the stakes are high. I know, as my grandson has ASD.
Michael Snyderman, MD
>So we are to believe that a specially brewed virus was born in a lab. It has no problem getting passed the immune system, but somehow never got there although it was not known it was infecting EVERYTHING they say it was for 15+ years. However, it ALWAYS gets into EVERY SINGLE POSITIVE sample in the positive studies but doesn't LOOK like those viruses and would never give positive results for EMs or serology assays, and it is integrated and replicating. LOL best fairy tale EVERRRRRRR.
>Anonymous @December 12, 2011 1:07 AM said…
"So why do you keep turning this place into the Cantina? You keep talking, not holding your peace." (This is in response to my previous comment in which I said, "…And apologies to Dr. Deckoff-Jones for yet another Star Wars Cantina Meltdown Cascade event. I shall hold my peace.")
This got me thinking about who was doing the talking. Using text-editing tools, a quick analysis of those posting so far on this current blog entry yielded:
Anonymous 101 56.42%
Jamie Deckoff-Jones MD 15 8.38%
Paula Carnes 13 7.26%
kathy d. 10 5.59%
Retrovirologist 9 5.03%
Jill 6 3.35%
AnonymousNonRetrovirologist 5 2.79%
fly 5 2.79%
Amy 2 1.12%
CFSBOSTON 1 0.56%
In Vitro Infidelium 2 1.12%
jace 1 0.56%
jillnz 1 0.56%
Lee Lee 1 0.56%
Michael Snyderman MD 2 1.12%
Nicky Reiss 1 0.56%
Peggy 1 0.56%
Samuel Wales 1 0.56%
shelley 1 0.56%
Wildaisy 1 0.56%
total posts 179 100.00%
So, as can be seen, unless my contributions are considered significantly more important to be weighted ~15x more heavilly than others', I cannot be held responsible for the majority of blood on the floor in this current Star Wars Cantina Meltdown Cascade event. Our numerous "Anonymous" posters represent a clear majority in this regard.
(I'd meant to somehow be able to associate comment word count with poster category–perhaps a better measurement of users' inputs– but that's a little too complicated to undertake right now and the Blogger HTML pages are too hard to parse in regards to associating comments with posters (at least not manually–perhaps if my unix-fu were stronger?)).
>@AnonymousNonRetrovirologist
I think you wish people to think this is a cantina, but star wars is fictional. Did you realise that?
So do you have anything to say now your numerous errors have been uncovered? Or do you intend to only make posts that are irrelevant to the topic?
>Does everyone realise that there are 3 positive MRV studies on ME?
The first (Grossberg) was published in 1997, but the findings made in 1989. That predates the 22Rv1 cell line by 3 years. I will try not to laugh.
The second it Lombardi and the third Lo.
>Detente already!
Lots of vested interests in being right. Why not use this energy to help people with CFS?
There are plenty of studies which show the prevalence of CFS in women at certain ages, mostly what's considered middle-aged.
Also, "fatigue" is a terrible misnomer. This is "fatigue" like a headache is comparable to pneumonia or one pimple is comparable to chicken pox. It is not "fatigue." Anyone who knows about CFS knows that. It is bone-deep unrelenting exhaustion which can leave one flat for days, unable to go outside, make meals, shower, go to the corner mailbox, etc. Some people are totally debilitated and can't even roll over in bed. Food has to be brought to them.
Anyone who professes to know a scintilla about CFS has to know that as a basic premise. But then again, people with this disease know it.
Others need to understand that.
There is a very moving post at Chronic Fatigue Syndrome Advocate by (our favorite name) "Anonymous" 3, by someone who is totally bed-ridden with CFS, can't go downstairs, can't shower, can't do anything, has to leave with the parents who help on everything.
That piece should be sent to everyone in the CDC, NIH, FDA, Dept. of HHS and to every Congressperson. It should certainly be read by everyone unfamiliar with the devastation of this disease.
>Correction in above post: The "Anonymous" 3 CFS sufferer has to live with parents who help on everything.
>This news is not a novel, it is a journalist's update on Dr. Mikovits and Dr. Lipkin's ongoing work. It will make your day and maybe make the whole rest of your life!!!!!!!!
http://www.cfsnovel.com/blog/?p=409
>I just read it. Is it confirmed???
I'm so excited I'm about to fly around the room lol!!!!
Love CrafterKate xxxxx
>Thank you so much, Paula, for posting that link. It is an uplifting news update about Drs. Ian Lipkin and Judy Mikovits, and Next Generation Sequencing.
And I hope the naysayers on this blog will hold their fire so that those of us with CFS can have some upbeat feelings for a few days about this!
>"There are plenty of studies which show the prevalence of CFS in women at certain ages, mostly what's considered middle-aged."
Most of those have used criterias that only require fatigue plus four minor symptoms. So they cannot be said to reflect the ME population as they use a mixed cohort, with many causes of fatigue in there including ME patients who's disesae doesnt respond to psychosocial treatments
>http://www.cfsnovel.com/blog/?p=409#comment-1009
I'm afraid this does not ring true. If it was correct and a proper study the design would be published on the NIH website. Why are people blindly going along with it? Lipkin has been chosen by Fauci of all people and has had a massive PR campaign around him this last year to make us think he could do no wrong. When did he find a retrovirus?
I am also not going to take anything that appears on the website of a patient. This has to be put on the NIH website with guarantees that all labs taking part use each others assays. You can't only have Mikovits and Ruscetti tested and we don't even know if it is true they are taking part. Mikovits is tied up in court and civil cases at this time.
We need them to state all assays will be clinically validated. That pedigreed negatives will be used. That those negatives will be thoughly prescreened by all labs, including PBMCs. No repeat of the blood study. We need to know exactly which labs are being included. We need to know that no VP62 assays or 22rv1 will be used as that is their continued excuse and not needed when assays should be optimised to a clinical positive. There should be no modifications to assays. The final paper should record what happened to the collection and blinding of all samples from all labs. And a promise to not give one set of patients to one lab and another to other labs.
If they can't do this the study is not valid at all. So when is the NIH page appearing?
>Ian Lipkin, Judy Mikovits, Frank Ruscetti and Next Generation Sequencing, and Paul Cheney's support – this is confirmation that the retroviral hypothesis is very much alive, was never dead, and validates our informed trust in Judy.
Shame on the Wantmore's for their lack of decency. The callous and calculated sacking of Judy is not how you thank the scientist who just saved your daughter's life! They could stop the legal torture, but its the entitled nature of the 1% to play the system in their favour. Time to close their fb page again!
Now back to the good news. I wish you a very Happy Birthday dear Jamie, you sage and savvy Sagittarian – your birthday wish has come true! You were our light in the dark and confusing times we were plunged into, our lifeline. "In Jamie we trust" too :)
Your *presence* has been the most valuable gift to the ME/cfs community, no material gift this silly season brings could ever compare with this! We love you dearly and treasure your fighting spirit.
Best news of 2011, I think I'm gonna need some champagne… Cheers Jamie and Judy!
A Starfish Downunder xxxxx
>I have not seen one thing about Cheney supporting this claimed NIH study with Mikovits and Ruscetti.
Nor is there anything about them doing deep sequencing. That is Lipkin, which is a conflict of interest if he were heading a study.
>Why is the NIH hiding the study design from patients and instead drip feeding what may not be true through patients?
>It is vitally important for the future of M.E. patients that there is complete transparency about the study design. The NIH should make this available now.
>I hope people are aware that Lipkin deep sequencing has nothing to do with the multi lab study. Cheney's comment was also separate to this multi lab study.
If these rumours are true and we need this on the NIH website according to the NIH's own guidelines and in the interst of transparency, then having only Mikovits and Ruscetti taking part is not a multi lab study.
They are in the same lab!
Also is this lab a mouse free lab? Was it ever used to experiment on mice?
If this goes ahead and they try to shut down research because the NIH messes up the design of the study it will be the only negative paper as everyone else has looked for the wrong viruses.
We cannot stop research when 2 positive studies exist and only 1 messed up negative study. We need a guarantee they will not stop research after 3 studies.
Also, why are other labs not involved?
>Hi Jamie, can you confirm if these details are correct?
Do Judy and Frank have a new lab?
are they visiting lipkin this month?
hope you can bring us some good news.
>Jamie cannot confirm. The details are only known to the NIH and they must outline the full plan on their site or what are they hiding?
If Judy and Frank are only taking part, they cannot confirm their own findings.
>@Anon December 15, 2011 5:40 AM
"If Judy and Frank are only taking part, they cannot confirm their own findings."
Sure they can. It is in fact one of the purposes of studies like this one. If ANYBODY (Mikovits/Ruscetti/Lo) can reliably differentiate between patients and controls, it would be BIG news all over the world.
And more importantly, if their initial results were true, they (or at least on of them) should really be able to differentiate between patients and controls.
It seems to me that you are finding it very unlikely that Mikovits or Rucetti or Lo will be able to reliably differentiate between patients and controls, and are therefore already making up all minds of (nonsensical) excuses.
First it was a problem that Mikovits wasn't participating (and I would agree), and now it's useless if she is participating because she "cannot confirm her own findings" anyway?
>@RRM
Ha ha ha
How many times have you stated. They cannot confirm their own findings. LOL now you change your mind.
They have already confirmed their findings then. In Lombardi et al. It was blinded and supported by multiple clinically validated assays.
Lo et al also confirmed the findings.
So there are two positive papers, and this new study that if design as the BWG paper was will not provide any results that are scientific. And this is how you wish to stop further research. LOL
Who's has said Lo is involved in the study? Another reason we need the NIH to publish the details on their site. Lo's team used the wrong assay in the BWG and not the one that worked in their own study. If they do this here, they will get predictably negative results. This is not science.
Firstly it was that they couldn't validate their results, and that they were the only ones taking part. Now you say they can and that Lo is taking part.
Publish the full study design on the NIH site, state they are using only clinically validated assays. And then it can go ahead. Not before.
>@Anon December 15, 2011 8:32 AM
"How many times have you stated. They cannot confirm their own findings. LOL now you change your mind. "
If you read correctly back on this blog, you'll see that I have posted BEFORE the results of the BWG study were out, that I would eat my words if ANY of the original labs could differentiate between patients and controls.
What I have explained multiple times however, is that the original study cannot be CONFIRMATORY of its own results. And while the samples were blinded (by the investigators themselves, which could still lead to biased testing), the patient and control samples WERE NOT handled exactly the same from collection to testing.
However, when an INDEPENDENT party collects and blinds patients and controls (which are handled IDENTICALLY from start to finish), then yes, the oriiginal lab can confirm its own results through picking the patients from the controls.
"And this is how you wish to stop further research. LOL"
You act if I have some power over this. I don't.
I'm just telling you that, in actual reality, if Mikovits (/Lo/Rucetti) are again unable to validate their original findings in freshly collected samples, using methods of their own choice, it's basically game over with the goverment funding the XMRV/HGRV story.
Of course, you'll be still crying foul then, but that's the way it is. If Mikovits is corect, we can expect her to reproduce her findings AT LEAST ONCE in two independently organized studies.
"Who's has said Lo is involved in the study?"
I am saying this. Although anything can of couse change, based on earlier statements by reliable sources, the testing will be performed by the Mikovits group, the Lo group and the Switzer group, each of course using methodology of their own choice.
Lo did not use the wrong assays in the BWG study. You can see in Fig. 2 of the Lo paper that the primers reported for the BWG study lead to positive results.
"Publish the full study design on the NIH site"
Ah yes, because that really happens all the time in science.
I would actually favor some public explanation about the set-up of this study but there is really nothing sinister about how it's being done.
"state they are using only clinically validated assays."
Again, you have made up this concept in your head, but it doesn't exist in the actual reality of validation studies. This way, you can disregard any study that doesn't report the results that you want.
In actual reality, all participants can use the methodologies of their own choosing. If you read Lipkin's paper on (de-)discovery studies, you'll see that this is his modus operandi when there is enough fundig to include multiple labs.
>@RRM
"If you read correctly back on this blog, you'll see that I have posted BEFORE the results of the BWG study were out, that I would eat my words if ANY of the original labs could differentiate between patients and controls."
You have always said they cannot confirm their own results. Now you are backtracking. Lol We don't have one clue who is taking part in the study still as it is not on the NIH website.
"What I have explained multiple times however, is that the original study cannot be CONFIRMATORY of its own results. And while the samples were blinded (by the investigators themselves, which could still lead to biased testing), the patient and control samples WERE NOT handled exactly the same from collection to testing."
Lombardi was confirmed by Lo.
The samples were handled the same way as Ruscetti and Mikovits stated in their response to comments in Science,
"However, when an INDEPENDENT party collects and blinds patients and controls (which are handled IDENTICALLY from start to finish), then yes, the oriiginal lab can confirm its own results through picking the patients from the controls."
The samples for Lombardi et al. were sent to Mikovits and Ruscetti blinded. Done already.
Contact controls will be more positive than the general population and patients selected by those who use criteria such as Fukuda will be lower than for CCC. As fukuda does not require people to have a neuroimmune disease. Where are the stated facts about those parts of the design on the NIH website?
"I'm just telling you that, in actual reality, if Mikovits (/Lo/Rucetti) are again unable to validate their original findings in freshly collected samples, using methods of their own choice, it's basically game over with the goverment funding the XMRV/HGRV story.
Of course, you'll be still crying foul then, but that's the way it is. If Mikovits is corect, we can expect her to reproduce her findings AT LEAST ONCE in two independently organized studies."
The BWG study had no pedigreed negatives, so every positive cannot be said to be incorrect, 22Rv1 was used in the CDC lab with some collection tubes, clinically validated assays were not used, Mikovits didn't do the BWG, Lo's team changed assays, no trizol was used defeating the WPIs assay. You can forget about the one study thing then. And if this repeated again we will see a duff study without any scientific basis.
"I am saying this. Although anything can of couse change, based on earlier statements by reliable sources, the testing will be performed by the Mikovits group, the Lo group and the Switzer group, each of course using methodology of their own choice.
Lo did not use the wrong assays in the BWG study. You can see in Fig. 2 of the Lo paper that the primers reported for the BWG study lead to positive results."
How do you know that when the NIH have not published it on their website? If this was a proper study all labs would use each others assays also. Why are patients being denied this information and why is Lipkin not saying put it on the NIH website?
Lo's team did use the wrong assay that didn't work. They did not use the one the results were taken from.
"Ah yes, because that really happens all the time in science.
I would actually favor some public explanation about the set-up of this study but there is really nothing sinister about how it's being done."
Then the NIH can post the full breakdown if they are hiding nothing.