
One morning an elderly man was walking on a nearly deserted beach after a big storm had washed up thousands and thousands of starfish. He came upon a boy who was picking them up and throwing them back into the ocean, as eagerly as he could.
Puzzled, the older man looked at the young boy and asked, “Little boy, what are you doing?”
The youth responded without looking up, “I’m trying to save these starfish, sir.”
The old man chuckled aloud, and queried, “Son, there are thousands of starfish and only one of you. What difference can you make?”
Holding a starfish in his hand, the boy turned to the man and, gently tossing it into the water, said, “It will make a difference to that one!”
It is all well and good to say that now that XMRV is dead, science can get back to its orderly, stepwise process; they even get to say, we told you so. And I say what I have said all along: millions of patients need treatment now. It is not a static situation. It is a progressive disease, slow, but lots of people are circling the drain. Many new cases that might be easier to treat sooner rather than later… that might respond more completely to arv’s. New babies being born with it. Should we wait a decade to start to find out, in a systematic way, if existing treatments might not affect it? It is incumbent upon the medical and pharmaceutical industries to think about the disease in concept and find solutions, not sit there doing nothing until Virus X is found; that approach already hasn’t worked for decades. It is quite likely that it won’t turn out to be a one virus, one disease, one treatment paradigm. If it were that simple, it would have been found already. So I find myself sitting with real patients, in the here and now, framing the illness as I have outlined here over the last year and a half. I still find the model we are evolving useful in a clinical context.
In my last practice, my interest was peak performance with respect to brain function, no matter the degree of injury or illness. I worked with the things that I found useful, personally and for my patients, most of whom had already exhausted their medical options. I was undiagnosed at that time. I knew I was sick, but it wasn’t too bad, and I knew that conventional medicine had nothing to offer me. It occurred to me now and then that I had some sort of less than MS. Other possibilities occurred as well. I tried to fit it into PTSD, but there were too many physical manifestations, hypertensive crises, arrhythmias, atypical migraines, malaise, this or that instability. I could exercise without problems for a decade. I used to say that whenever something went wrong with my body, it was undiagnosable. And I was CFIDS aware. That state of not knowing made me well suited to being a doctor of last resort. My armamentarium then was HBOT, neurofeedback, nootropics (cognitive enhancers), nutraceuticals, herbs and bioidentical hormones. I found discontinuing unnecessary drugs to be a powerful treatment modality. And I tried to create the space for the less tangible, but no less powerful healing that can happen in the context of connection and relationship.
So far, I am using pretty much the same gentle, yet powerful modalities that I used before, when I didn’t know what I was doing:), and I’m having some beginner’s luck. I am turning to these treatments first, because I know from experience, they work, and now I have a framework that gives me a better idea why. Pulsed, high dose normobaric oxygen is the most powerful and easy to deliver treatment that I have to offer. My patients so far are pretty uniformly impressed. Nobody that has rented a concentrator for a month has returned it, unless to buy one. Responses range from a little helpful to “wow”. There is a short term effect and a long-term additive effect, as I observed with HBOT in practice. It seems one of the craziest things in all this that such a simple thing has been denied us. I wonder about why, and can’t come up with much. It will never be studied, because it can’t be patented. It might accelerate aging, but the longevity folks think it’s the opposite. It needs to be more carefully dosed for patients with seizures and a few other things. Mostly, it’s probably because doctors don’t understand the gas laws, and so are uncomfortable with it. They can handle it when it comes out of a wall in a hospital, where it’s use is sanctioned, and there’s a respiratory therapist to hook things up. Otherwise, if you have COPD or are dying, you can have it. Sometimes insurance will cover it for cluster headaches, or migraines, common in our patient group. I am prescribing oxygen, for an hour a day and prn, at 10L/min by non-rebreather mask (has a reservoir and check valves), or 5-6L/min by simple mask for patients who bought lower flow concentrators (two are improving with this).
Here are a couple of references that address the oxygen paradox: Why might high dose oxygen be good for us, even though we have increased oxidative stress at baseline?
Oxidative stress, antioxidant defenses, and damage removal, repair, and replacement systems. Davies: Cells, tissues, organs, and organisms utilize multiple layers of antioxidant defenses and damage removal, and replacement or repair systems in order to cope with the remaining stress and damage that oxygen engenders. The enzymes comprising many of these protective systems are inducible under conditions of oxidative stress adaptation, in which the expression of over 40 mammalian genes is upregulated.
HIV: reactive oxygen species, enveloped viruses and hyperbaric oxygen. Baugh: ROIs repeatedly have been shown to be virucidal against enveloped-viruses, like the human immunodeficiency virus (HIV). Hyperbaric oxygen therapy (HBOT) increases the production of ROIs throughout the body, leaving no safe harbor for the virus to hide outside the genome. This technique already has been tried on acquired immune deficiency syndrome (AIDS) patients, with exciting results.
As I am finishing my first six months of practice, Ali is coming into her own, with great courage. She has enrolled for an online undergraduate program at U Mass, and will start next month. She has been dating, but still mostly staying home rather than venturing out. Right now, she is deep in the process of confronting that she is probably physically able to do more things away from home, but confined by habit and the limitations of the past. It is hugely more difficult for her than for me to emerge, without a former life to go back to.
Ali credits oxygen and modified Meyer’s cocktail infusions with her slow but continued improvement. She tells me when she feels the need for an infusion. We are still tinkering with the best formula for her. She uses oxygen 4-5 times a week, according to her own instincts. She has come to use it prophylactically for PEM, when she knows she’s overdone it. It is impossible to know what role antiretrovirals are playing in maintaining her gradual improvement which began with the cessation of Lyme treatment and was also obviously impacted by Deplin and treatment for PCOS (polycystic ovarian syndrome). Our concentrator has been broken for a couple of weeks and when the replacement came, she grabbed the mask, exclaiming “Oxygen! Mana of the Gods.” For me too, oxygen is the most tangible thing I have. It impacts my sleep directly.
 |
| click to enlarge |
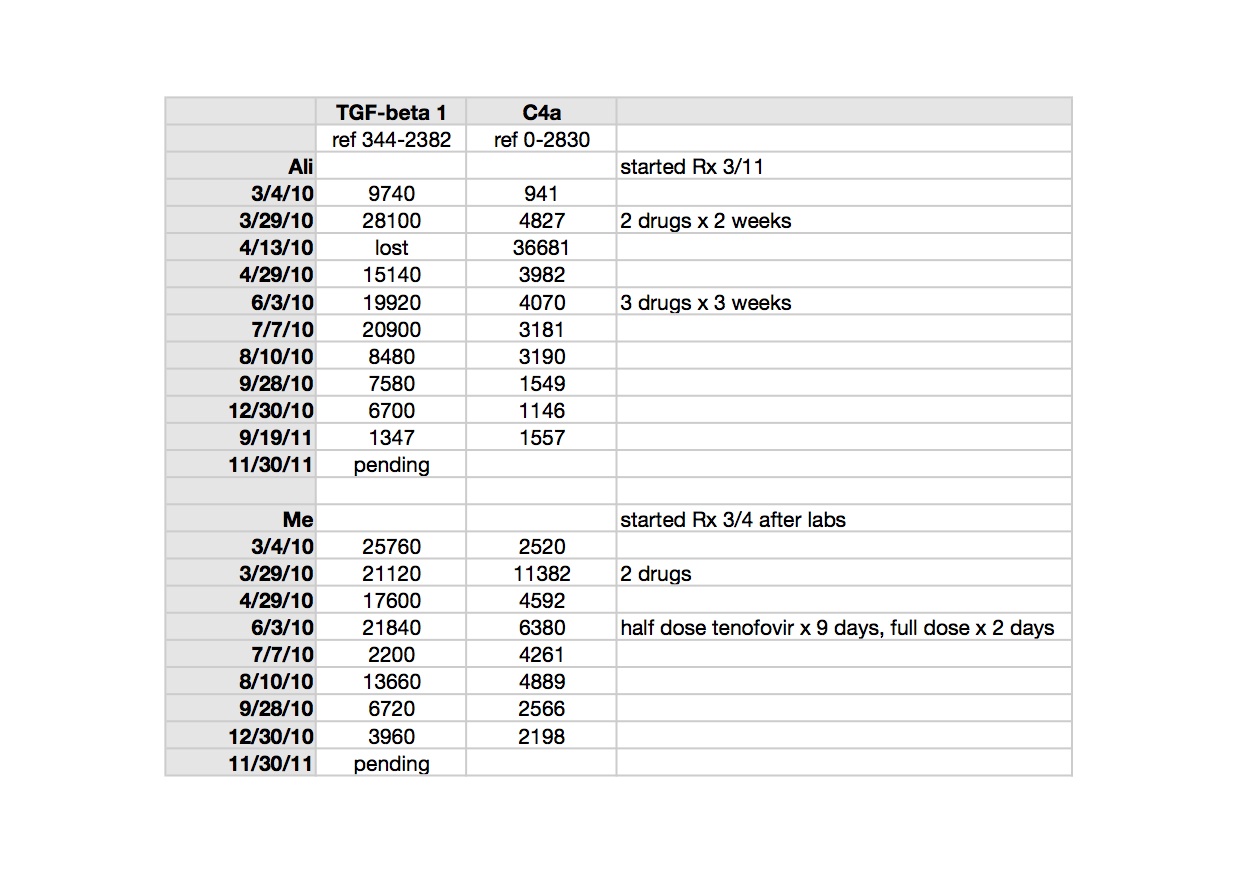
TGF beta-1 is a peptide involved in many cellular functions, including the control of cell growth, proliferation, differentiation and apoptosis. Here is a recent paper suggesting TGF beta-1 as a marker for CFS: Up-regulation of TGF-β1 mRNA expression in peripheral blood mononuclear cells of patients with chronic fatigue syndrome. Zhang. It is tempting to speculate that TGF beta-1 could be involved in the clonal expansion we are starting to think about with respect to the pathogenesis of ME/CFS and related leukemias; not forgetting that simple animal retroviruses replicate mitotically, by clonal expansion.
TGF beta-1 is implicated in the pathogenesis of Marfan’s Syndrome, which my husband’s uncle, husband and son have; in our family it appears to be more obviously expressed in each successive generation. Elevated TGF beta-1 is implicated in the pathophysiology of Marfan’s. My husband and I both had different, subclinical manifestations of illness when we met, but most, though not all, of his were attributable to Marfan’s. Marfan’s is an autosomal dominant genetic condition where chromosome 15 encodes for a defective protein which is necessary to bind TGF beta-1 to keep it sequestered to normal levels (oversimplified model). Losartan, an ARB (angiotensin receptor blocker) has been shown in clinical trials of Marfan’s patients to lower TGF beta-1 and slow the onset of the most serious consequence of the disease, aortic root dilatation. My biological father had a body habitus consistent with Marfan’s and I may be an Ehlers Danlos variant, becoming more flexible with age and exacerbations of illness. I have minor features of both conditions. Both Marfan’s and Ehlers Danlos seem to be over-expressed in the ME/CFS patient group, already showing up in my tiny practice. Here is an excellent article which considers related disorders with respect to abnormal TGF beta-1 signaling: Transforming growth factor-beta signaling in thoracic aortic aneurysm development: a paradox in pathogenesis. Jones/Ikonomidis.
>@ Retrovirologist,
It is very encouraging that you are thinking about it this clearly, except for the fraud part, which I think the least likely explanation for where we are now. Too much smoke. It is wonderful to hear that Dr. Lipkin is considering retroviruses in his search for a viral etiology. I was hopeful when I met him that it would catch fire for him. We would all love to know who you are, but understand the reasons why you might not want to tell us. Thank you for sharing your thoughts nevertheless.
Best,
Jamie
I would love it if you would back channel me. I swear I won't tell who you are:). jdeckoffjones@gmail.com
>"on the day when Don Ganem and his lab were scraping the wells from their Virochips from RNASEL mutant samples, maybe someone was working with 22Rv1 (or other contaminated line). "
Is this the next joke then? Pretend it was 22rv1?
The problem being 22rv1 hasn't been shown to be infected with anything but vp62, which was made by Silverman post testing in 2006!
>I'm tired of arguing with you. You are missing my point completely. Here is what I wrote way up:
"An SU antibody primarily reacts with the SU protein of SFFV and can cross react with other SU proteins. This includes MLVs."
Honestly, I don't even know why you are arguing. Think about it. I stated that the SFFV ab can react with other MLVs. This is exactly what you are saying too. Here:
"SFFV will only react to the SU protein of an MLV."
We (well really you) are arguing about the same thing. So I will agree with you:
YES, an ab to SFFV will react to MLV SU proteins. YES! YES!!!! LOL….
But here is what I'm saying in addition. Because there are so many MLVs and ERVs that could react with that antibody, its really unknown what will. And its impossible to say that XMRV antibodies were produced in mikovits paper. What if it was another MLV?
And what the heck are you talking about HTLV??? lol….
>An ERV cannot react to this antibody as again you should know if you are a retrovirologists. It relies on the SU protein. The viruses detected are MLV-related, and not ERVs. You can't say another MLV-related virus when they are MLV-related viruses that have been discovered.
Trying to make nasty claims about the research to tear down Dr Mikovits and Dr Ruscetti, you may as well be trying to destroy evidence for HTLV, the virus he discovered. Don't act like a snake.
You do realise real people are at the end of this? Real children who are and have died? Fraud or real a scientist would not be here desperately trying to talk patients out of finding the truth, they would be in the lab using clinally validated assays on a set of me patients selected with neurological signs and symptoms. Have a look at what happened to Alison hunter or Lynn gilderdale and try giving an excuse that you can do nothing.
>Jamie,
Thanks for the support but the anon poster, whom I like to affectionally call the "clinically validated ASSay", makes it abundantly clear that exposing my identity will be foolhardy.
Its pretty clear he or she is hell bent on attacking me and basic science fact. He could be misleading your readers and I would consider stronger measures of censorship.
As for back channels – your spat with Jason was most unfortunate and the main reason why I won't do this. I definitely think Jason went too far in his stance in attacking you and was totally uncalled for. However, I know him. he's a good guy and superb scientist. I'm pretty sure he was reaching out to you and the community.
>@ Dr. Retrovirologist,
Censorship is not my thing, pretty clearly:).
I'm sure Jason is a nice guy. Professor Racaniello too. But they both need some sensitivity training; maybe too much time in the lab:). Also your entire community needs to stop trying to call the shots for patients, without knowing the first thing about the disease. It has really been an amazing display of arrogance and being out of touch with the needs of the people the work is supposed to be helping. Or if it's not about the people, then why not stick to what you do and don't know about viruses. My speculating about your work doesn't have the same potential negative impact on patients as your speculating about mine. I don't understand why a scientist wouldn't be frightened to make statements that result in shutting down treatment options for suffering people. Heavy responsibility to take on, just because the first X you looked for wasn't it.
Jamie (happy to discuss it whether you are anonymous or not)
>Do bloggers really think that total war would ensue if identities were revealed? This is a discussion about research, differences of opinion, yes, but nothing lethal.
Why is it going on with such vitriol continually? Can't a scientific discussion take place without that?
It's very off-putting to see this occur again and again.
Can't people have discussions without this dormant, then overt hostility? What gives?
I'm sick. I'd very much like to see the cause found. I'd like to see treatments found.
What is all of this arguing in this tone contributing to knowledge which will help CFS sufferers? How will we be helped by this?
Or is it just different people staking nearly life-and-death claims?
I would just like the clearest explanations possible for those of us who are not retrovirologists or other types of researchers.
Is that too much to ask for those of us who have have this disease on our backs for years?
>Retrovirologist I do hope you are able to compete a reply on the other half of my questions – I guess that is 1.5 questions remaining.
I am sorry I don't have time to study all this tonight, but will get to it hopefully tomorrow. My only additional thought before I chill a bit is that RNaseL is very abnormal in CFS patients. I would assume that is the EFFECT of some infections, possibly retroviral, not the defect that opens the door – not the CAUSE. That is why I mentioned it and bothered to post a lengthy portion of DeMeirleir's book.
Anaon wrote:
RNaseL has no influence on who is infected with MLV-related viruses. This was proven in Singhs positive prostate cancer study, the one that used different assays to her ME study.
>Paula Carnes @December 8, 2011 10:54 PM said…
"Hello NonRetrovirologist: What did that germ turn out to be – the one you were working with in the 1980s? I am just curious."
Paula: "non-A/non-B hepatitis" was the provisional name given to Hepatitis C, up until Dr. Alter et al. isolated and characterized it. (I was part of a team that helped isolate some early HepC samples for the first PCR diagnostic tests–I was just out of school and I was just another pair of hands back in those days– I worked cheap and was expendable!)
" As to Dr. Lo his work on mycoplasma….Have you read his original findings of mycoplasma fermentans (incognitus strain)? I don't know that the study is online. I should post it on my website. It describes six dead bodies brought to his lab. He determines that they all died in about 6-8 weeks from a virus-like infection. The only ones who lived a few more weeks were put on antibiotics. When they were taken off the antibiotics they ALL DIED. It turned out the virus-like infection was mycoplasma incognitus."
No, I did not know this about Lo and his earlier work, only that he had proposed mycoplasmas as a possible cause for AIDS and later on, for CFS. My experience with mycoplasma is as a cell culture nuisance, not a human pathogen. Do post the reference on your website, I'd like to read it.
"I have mycoplasma incognitus. How come I am still alive? Go figure. There are a lot of mysteries about CFS, aren't there?"
That's why I don't think any repudiation of the Lombardi/Mikovits' XMRV/MLV work on CFS will keep people from continuing work on the syndrome(s). Dr. Lipkin's suggestion (something along the possibility of it being "normal virus or viruses interacting with an abnormal immune system") may turn out true. The Norwegians with their Rimixutab may have demonstrated an autoimmune contribution to the syndrome. It's still a wide-open field for study.
"I hope he (Dr. Lo) continues to work on this murine retrovirus mystery."
Even if there are no more contributions from his lab, there will be from others. (People may just have to be ready to accept conclusions and results that they may not like.)
(And apologies for delayed reply–have been travelling and without a reliable internet connection.)
>The poster calling him/herself "Retrovirologist" has been doing a fine job explaining the scientific issues, the interpretations of various results cited, and the how's, why's and what's of the various techniques used and should be thanked for taking the time to contribute to this blog. I appreciate his/her commentary. The expertise being offered up here should be welcomed. I think most experts avoid engaging with "civilians" on the Internet because, as many of the responses show (here and elsewhere), it usually doesn't end well.
It is said that on the Internet, no one knows you're a dog. But even on the Internet, it's still possible to tell if it's been doing molecular biology, and if it hasn't.
And apologies to Dr. Deckoff-Jones for yet another Star Wars Cantina Meltdown Cascade event. I shall hold my peace.
>> (People may just have to be ready to accept conclusions and results that they may not like.)
That sounds disparaging of advocates.
I hope you didn't mean that.
>Retrovirologist,
Still haven't caught up on reading here. I might have figured you worked on hep C. There is a good scientist, Gail Cassell, working now for Eli Lilly but used to work at U. of Alabama who is one of the top researchers in the world on mycoplasmas. Her articles on links between infections and autoimmune diseases is significant.
I spoke on the phone with Dr. Lo several years ago. He impressed me as deeply concerned as to what CFS is. But I think all have agreed that mycoplasma is not the CAUSE of cfs anymore than it was or is the cause of AIDS. It certainly plays a role as a cofactor, but not a necessary cofactor anymore than EBV etc would be. Here is the abstract of Dr. Lo's work with a few extras I added from the entire published study. I do not think that is available online.
Let me point out the curiosities which are found in the entire article but not in the abstract. The six bodies came from six cities were there are US military bases. Their deaths were reported one month at a time all in the same year. The deceased were black, white, male and female, and all under age 40. The one who lived 7 weeks was given doxycyline while in the hospital but died after leaving the hospital and doxy was stopped when the infection worsened. After Lo wrote and published this article he later realized this was a new mycoplasma and named it "incognitus." One can see where conspiracy theories might come to mind. Why did these people die in these locations and on a monthly schedule from a pathogen that turned out to be a cell wall deficient bacteria? – Paula Carnes
American J. Trop. Med. Hyg. 41(3) 1989 pp 364-376 (9-098)
Copyright 1989 by The American Society of Tropical Medicine and Hygiene
ASSOCIATION OF THE VIRUS-LIKE INFECTIOUS AGENT
ORIGINALLY REPORTED IN PATIENTS WITH AIDS
WITH ACUTE FATAL DISEASE IN PREVIOUSLY
HEALTHY NON-AIDS PATIENTS
SHYH-CHING LO, MARILYN S. DAWSON, PERRY B. NEWTON III,
MARY ANN SONODA, JAMES WAI-KUO SHIH, WLATER F. ENGLER
RICHARD YUAN-HU WANG, AND DOUGLAS J. WEAR
American Registry of Pathology, Armed Forces Institute of Pathology,
Washington, DC;
and Warren Grant Magnuson Clinical Center, National Institutes of Health,
Bethesda, Maryland
Abstract: We studied 6 patients from 6 different geographic areas who
presented with acute flu-like illnesses. The patients developed persistent
fevers, lymphadenopathy or diarrhea, pneumonia, and/or heart, liver, or
adrenal failure. They died in 1-7 weeks. These patients had no serological evidence of HIV infection and could not be classified as AIDS patients according to CDC criteria. The clinical signs as well as laboratory and pathological studies of these patients suggested an active infectious process, although no etiological agent was found despite extensive infectious disease work-ups during their hospitalization. Post-mortem examinations showed histopathological lesions of fulminant necrosis involving the lymph nodes, spleen, lungs, liver, adrenal glands, heart and/or brain. No viral inclusion cells, bacteria, fungi, or parasites could be identified in these tissues using special tissue stains. We report that immunohistochemistry using rabbit antiserum raised against VLIA, the virus-like infectious agent previously identified in patients with AIDS and shown to cause fatal systemic infection in primates, revealed VLIA antigens in those necrotizing lesions. In situ hybridization using an S labeled VLIA-specific DNA probe also detected VLIA genetic material in the areas of necrosis. Furthermore, virus-like particles closely resembling VLIA were identified untrastructurally in these histopathological lesions. VIOA was associated with the systemic necrotizing lesions in these previously healthy non-AIDS patients with an acute fatal disease.
>"Its pretty clear he or she is hell bent on attacking me and basic science fact. He could be misleading your readers and I would consider stronger measures of censorship.
As for back channels – your spat with Jason was most unfortunate and the main reason why I won't do this. I definitely think Jason went too far in his stance in attacking you and was totally uncalled for. However, I know him. he's a good guy and superb scientist. I'm pretty sure he was reaching out to you and the community."
"could be misleading" – as in not misleading. Somehow that has fallen to yourself. Another impostor hoping to convince others without providing one piece of evidence and using the same old tricks that the Wessely school do to turn it into a them and us, when the situation is viruses versus humans.
If you are anything that you claim and there is no indication you are, I'm sure your family and friends won't thank you in the future for exposing them to these viruses and the diseases associated, but as long as financially you are safe…not a problem.
>"Why is it going on with such vitriol continually? Can't a scientific discussion take place without that?
It's very off-putting to see this occur again and again.
Can't people have discussions without this dormant, then overt hostility? What gives?"
Kathy, I prefer to be attacked upfront then stabbed in the back as these posters like to do. They want you to think they have qualifications but cannot reveal who they are as their comments would backfire on them if they were working in the field. They also fail to provide any little bit of evidence to support their lies.
"I would just like the clearest explanations possible for those of us who are not retrovirologists or other types of researchers."
The evidence is for the viruses as causative.
>"That's why I don't think any repudiation of the Lombardi/Mikovits' XMRV/MLV work on CFS will keep people from continuing work on the syndrome(s). "
Who would even suggest it would, but that has been the reality for many years now. Can't say the last two years have changed anything, not as if virologists have bothered to conduct science when looking for the viruses. They are happy to leave the dying patients to psychiatrists hands and destroy their own field. What a fantastic world this will create.
"(something along the possibility of it being "normal virus or viruses interacting with an abnormal immune system") may turn out true. The Norwegians with their Rimixutab may have demonstrated an autoimmune contribution to the syndrome. It's still a wide-open field for study."
The Norwegians have produced further evidence to support that MLV-related viruses cause autoimmune symptoms in ME.
"Even if there are no more contributions from his lab, there will be from others. (People may just have to be ready to accept conclusions and results that they may not like.)"
Are you saying Lo does not feel it is now safe? Thanks for letting the sick and dying know how scared everyone is.
>@AnonymousNonRetrovirologist
"The poster calling him/herself "Retrovirologist" has been doing a fine job explaining the scientific issues, the interpretations of various results cited, and the how's, why's and what's of the various techniques used and should be thanked for taking the time to contribute to this blog. I appreciate his/her commentary. The expertise being offered up here should be welcomed. I think most experts avoid engaging with "civilians" on the Internet because, as many of the responses show (here and elsewhere), it usually doesn't end well."
LOL really! I would like some proof you are both what you claim to be, but I know you won't be doing that. I would also like to see some responses with evidence from you two, but I know you won't be doing that.
"It is said that on the Internet, no one knows you're a dog. But even on the Internet, it's still possible to tell if it's been doing molecular biology, and if it hasn't."
I can see you and retro have stayed well away from science in general.
"And apologies to Dr. Deckoff-Jones for yet another Star Wars Cantina Meltdown Cascade event. I shall hold my peace."
So why do you keep turning this place into the Cantina? You keep talking, not holding your peace.
Patients are used to this.
>The only apology that a scientist need make is for departing from the scientific mode of investigation and seeking to provide evidence which supports their preconceptions. When that happens published studies which appear to portray scientific content actually portray nothing but the opinion of the researcher.
No other entity can react with a monoclonal antibody to sffv env. This is why it was used.
The evidence from the four seperate experiments proves beyond reasonable doubt that the entity was a replicating MuLV class gammaretrovirus. The new env sequences show that it was not related to the sequence VP-62.
>I am worried I have already or may in the future pass a retro virus onto to my children and grandchildren.
what about pets, cats and dogs?
Can anyone tell me that it is safe for them all to have close contact with me?
The sort of contact where they might pinch my cuppa tea, finish my apple or biscuit.
Run off with my freshly used toothbrush.
The sorts of things you cant always control for,
what precautions should WE be taking.
What partners, are they likely to have it already, or should they follow the same precautions I should.
What about my ASD daughter, is it safe for her to have close contact with her nieces and nephews?
These questions are never far from my mind, these questions are the ones I want answered most urgently.
>@fly, a large and growing list of some of the top institutions and virologists in the world have said that XMRV is a lab contaminant, does not cause ME, and poses zero risk to the blood supply. No one knows what causes ME, but if you want to spend the rest of your life avoiding your loved ones and pets just because a bunch of loony, angry non-scientists insist otherwise, that is your choice and yours alone.
>Hi Anonymous,
As far as I can tell, you did not answer fly's question.
As far as I can tell, she didn't ask about XMRV.
Are you saying that you did and she did?
Is the answering of a question about one thing by talking about another thing intended to demoralize?
Would you put your name to your reassurance?
>Retrovirologist,
is it possible the infection lo identified eventually as a mycoplasma was actually a new retrovirus in humans? I recall there was discussion about this at the time. In any case it is bizarre that these folks died, responded to doxycycline and came from the US and other countries the same year.
>@fly
A small heard from group of virologists have used their gut feelings to inform their mouths it is contamination. They have however provided no evidence.
The blood supply has not been screened, only 14 patients with no controls have using VP62 assays. Therefore it is impossible to declare the blood supply as safe.
"just because a bunch of loony, angry non-scientists insist otherwise, that is your choice and yours alone."
Just because Alter, Lo, Hanson, Singh, Silverman, Cabrera, Mikovits, Ruscetti, Switzer and Coffin have all found these viruses. MLV viruses are also transmitted in saliva.
Anon, very silly to think you and yours cannot catch what you don't understand when people with all sorts of diseases are showing up with these viruses. Maybe you think you have access to treatment, but what happens when the disease changes and the budget no longer meets those demands?
>@Anon 1:15, I suppose I could spend all day worrying about being struck by lightning or an steroid hitting the earth and wiping out mankind, but I choose not to.
>WOW are steroids really that dangerous?
>@Anon 1:15, I suppose I could spend all day worrying about being struck by lightning or an steroid hitting the earth and wiping out mankind, but I choose not to.
So why hand around with patients then?
The risk of a lightening stick is small. MLV-related viruses are being found in 3-7% of the general population with first generation testing.
>"I suppose I could spend all day worrying about being struck by lightning or an steroid hitting the earth and wiping out mankind, but I choose not to."
If we take the blood of a person found to be infected by Mikovits and Ruscetti and then use an assay of your choosing from the negative none clinically validated assays. Would you take their blood?
>http://www.virologyj.com/content/pdf/1743-422X-8-531.pdf
Downregulation of APOBEC3G by Xenotropic Murine Leukemia-Virus Related Virus (XMRV) in Prostate Cancer Cells
"Conclusions
We propose that XMRV replicates efficiently in prostate epithelial cells by downregulating A3G expression. Given that XMRV lacks accessory proteins such as HIV-1 Vif that are known to counteract A3G function in human cells, our data suggest a novel mechanism by which retroviruses can counteract the antiviral effects of A3G proteins."
"In the absence of Vif-like accessory proteins, retroviruses such as Human T cell lymphoma virus (HTLV) and Murine leukemia virus (MLV) have developed alternative mechanisms to evade host restriction by A3 proteins."
This virus is not VP62/XMRV. The viruses found in ME are also not VP62/XMRV.
>MLV-related viruses are not found in 3-7% of the general population, and yes I would have no hesitation in taking blood from a Mikovits + and everyone else – patient.
>MLV-viruses have been found in the following rates in the general population.
Lombardi et al. at 3.7%
Lo et al. 6.8%
Schlaberga at 4%
>"MLV-related viruses are not found in 3-7% of the general population, and yes I would have no hesitation in taking blood from a Mikovits + and everyone else – patient."
What does that mean? A patient found positive by Mikovits and Ruscetti. What is a Mikovits +?
Lets arrange it then and you have to sign something to say you are not taking ARVs or immune modulators.
>Retrovirologist,
I do hope you are still reading here as time allows. I have taken a look at your replies to me and have further questions. Thanks.
“some labs used the exact same protocols as Mikovits and did not find anything”
Which labs were these?
I understand your concept that studies need to have slight differences to validate the whole, but I tend to disagree in the case where a retrovirus may be very difficult to spot in blood and slight errors in handling or products used in testing could negate findings.
“In my opinion, if RNASEL was that important, why didn't they find other viruses? Also, the connection of RNASEL and CFS is tenuous at best and I can expand on this further if you like.”
Given that CFS patients are infected with multiple infections (HHV6, EBV, mycoplasmas, c. pneumonia, etc, both viral and bacterial, and that many of them have dysfunctional RnaseL, yes I would be most interested for you to expand on this.
“One is the very unfortunate possibility that she committed scientific fraud.”
Highly unlikely. Even if she is wrong, I think she is honestly wrong, not deliberately lying. For one thing, I think she is too smart to perpetrate such a stupid lie. Neither does she appear as a smooth talking con artist, quite the opposite, and I have seen a few of both.
“Specifically, I would like to see more studies looking for PMLVs in humans. Also, I definitely know that Lipkin is continuing to look for retroviruses in CFS samples as well.”
You wrote a bit about blood samples developing antibodies to something in the samples, but maybe not XMRV. Does it really matter what the retrovirus is exactly if the blood samples were developing antibodies? Wouldn't that indicate that the particular person had a retrovirus of some sort in his body already – potentially a retrovirus that could be making him sick? Are you saying that blood could develop antibodies to a lab contaminant because the lab contaminant was so closely resembling a virus already in the patient's body? Wouldn't that still mean the patient was INFECTED WITH SOMETHING BAD????
>@Anon at 2:31 pm
You do not want blood from us sickies. We are likely infected with something. We have enlarged lymph nodes, constant sore throats, extreme fatigue, abnormal weight gain or weight loss, brain confusion and abnormal immune function. Family members who are not blood relatives tend to also be getting sick. We are probably contagious at a low level. Do we have a murine retrovirus? Maybe not, but we have something that should not be donated to others.
>@Paula
"Which labs were these?"
None have replicated.
"I understand your concept that studies need to have slight differences to validate the whole, but I tend to disagree in the case where a retrovirus may be very difficult to spot in blood and slight errors in handling or products used in testing could negate findings."
Multiple assays have validated the positive results in multiple labs and papers. Replication is still a basic tenant of the scientific method.
"Highly unlikely. Even if she is wrong, I think she is honestly wrong, not deliberately lying."
There are many people also finding the viruses and DR Ruscetti has his name on the paper. It is equally his study also. Ruscetti did do all the WBs.
"You wrote a bit about blood samples developing antibodies to something in the samples, but maybe not XMRV. "
The antibody used can only detect an exogenous MLV-related virus. No evidence exists to say differently.
"You do not want blood from us sickies. We are likely infected with something. We have enlarged lymph nodes, constant sore throats, extreme fatigue, abnormal weight gain or weight loss, brain confusion and abnormal immune function. Family members who are not blood relatives tend to also be getting sick. We are probably contagious at a low level. Do we have a murine retrovirus? Maybe not, but we have something that should not be donated to others."
Yes, sad that people are really that silly. Jail is the outcome for anyone trying this with HIV. Jail is also the outcome for using assays not clinically validated to detect HIV.
>"Jail is also the outcome for using assays not clinically validated to detect HIV."
What about unvalidated assays for XMRV?
>"What about unvalidated assays for XMRV?"
Exactly the point! Now you agree it is unnaceptable to not clinically validate. What you cannot be protected from is others you encounter who are also infected. MLVs are transmitted in saliva – will that be also true for MRVs?
>"Exactly the point! Now you agree it is unnaceptable to not clinically validate."
Has anyone gone to jail so far in this whole affair?
>Just speaking for myself of course, I'm more worried about contracting the rage virus from 28 Days Later than I am people infected with MLVs.
>"Just speaking for myself of course, I'm more worried about contracting the rage virus from 28 Days Later than I am people infected with MLVs."
28 days is fiction.
"Has anyone gone to jail so far in this whole affair?"
Looks like your not keeping up. Why do you think assays for HIV must be clinically validated?
>"28 days is fiction."
And XMRV?
Dr. Simmons stated the BWG’s conclusions on XMRV starkest terms
“Certainly XMRV itself is a laboratory contaminant that was created in a lab by passaging through mice”
So not fiction, just a real live laboratory contaminant.
And that is why I'm more afraid of rage virus, however fictional, than I am of a known lab contaminant.
>"And XMRV? "
No one claims these viruses are fiction. The ME viruses are not shown to be VP62, or prostate cancer XMRV, and the new sequences in the genbank show some are polytropic.
"Dr. Simmons stated the BWG’s conclusions on XMRV starkest terms"
Stark is a word, not evidence. There is no evidence if contamination, and beliefs cannot be substitutes.
You are afraid of a fictitious virus called rage – well ok then, good luck with that. Zombies too?
>"You are afraid of a fictitious virus called rage – well ok then, good luck with that. Zombies too? "
Again yes, more so than XMRV, or MLVs, or gamma, alpha, beta, theta- whatever the dreaded new retroviral excuse for the latest negative study may be. Yes, zombies are far more frightening. Why not? The fictional threat you don't know is more scary than the lab contaminant that you do.
>You who are saying you're more afraid of a fictitious virus than a real disease — is this for real?
You must not be sick with this dreaded disease or any other or have a close relative do afflicted or you wouldn't say that. You'd want a cause to be found and treatment, and you'd encourage the research.
It is insensitive to make these cracks to those of us who live with CFS every hour of every day, and whose lives are ruled by it. Can't you see that at all?
You really don't want to get this disease or any long-term, permanent viruses or immunological diseases. But don't insult those of us who have it and want to see causes and treatments found — and not take 20 years either.
Let's not talk about jail. If we do that, I could ask why didn't the CDC researchers who diverted funding for CFS to other projects get punished for that? That was more than neglect. That was willful conduct, which harmed a whole class of people with CFS.
David Tuller reviews the sorry history of the CDC in its neglect and inaction on CFS in the recent article. He gives facts, quotes, information on this.
I think some folks should have lost jobs and seniority rights and been penalized for this. Maybe they should been sent to clean hospitals where people with chronic illnesses and immunological diseases are hospitalized. That, rather than the lofty jobs of research might give them a reality check of dealing with real, sick people.
>@anon December 12, 2011 11:20 AM
I don't have to avoid my family members you see they are all sick. Out of 8 of my immediate family members 7 have developed either cancer or a neuroimmune disease. These include MS and Parkinson's. Hope yours and other families will be luckier. Never say never as it can happen to you or a family member near you.
>"Again yes, more so than XMRV, or MLVs, or gamma, alpha, beta, theta- whatever the dreaded new retroviral excuse for the latest negative study may be. Yes, zombies are far more frightening. Why not? The fictional threat you don't know is more scary than the lab contaminant that you do."
Zombies are fictitious.
No evidence of lab contamination.
>"Since the predicted recombinant is ancestral to all XMRV isolates, and cannot have arisen more than once, it must have found its way into many laboratories as the 22Rv1 cell line was distributed worldwide and, by means that remain to be worked out, into clinical samples from CFS patients." – Coffin
Snigger!
That's too funny.
This isn't
Detection of MLV-like gag Sequences in Blood and Cell Lines Incubated With Plasma From CFS Patients and Controls
Systemic Immune Activation in XMRV Positive CFS/ME Patients
Detection Of Anti-XMRV Antibodies In Serum of CFS Patients and Healthy Blood Donors in Belgium
Health/Performance and Response Status of XMRV/pMRV Antibody Positive vs. Negative Chronic FatigueSyndrome (CFS) Subjects in a Phase III Clinical Trial
”There is increasing concern that in modern research, false findings may be the majority or even the vast majority of published research claims…Conflicts of interest are very common in biomedical research, and typically they are inadequately and sparsely reported…Prestigious investigators may suppress via the peer review process the appearance and dissemination of findings that refute their findings, thus condemning their field to perpetuate false dogma. Empirical evidence on expert opinion shows that it is extremely unreliable…Highly prejudiced stakeholders may even create a barrier that aborts efforts at obtaining and disseminating opposing results…” – Ioannidis JP. Why most published research findings are false.
>The papers listed above can be seen at this link
http://www.iacfsme.org/LinkClick.aspx?fileticket=%2BG6GTkbP33I%3D&tabid=499
>MS ASD ME FM MCS even a rare lung cancer strongly linked to SV40, are present across my family.
including non blood relatives.
something is crippling my family, but worse than that is the 'experts' who dont know the disease,keep telling us there is no link.
kids are going to be forced into CBT and GET to get them back into school, they are hoping to roll this out across the NHS for all diseases, and the USA have already bought into what the UK gov is selling.
any scientist worth his salt would put some effort into finding the problem.
NOT just turning up to knock down the only 'sensible explanation' that has been tabled since Defretas was destroyed.
Mr Retrovirologist,
why dont you focus on helping us to find out what is causing this disease.
and just a little curious, when did you first pay any attention to this disease?
Would you even be here with all yr expertise if Judy hadnt found a retrrovirus in us?
Yr interest is egoltistical and professional, our is survival.
Please DO find the cause, but please understand with the little understanding you show of the disease process and how little knowledge you appear to have about the many biomedical papers that have been produced.
It is you that needs to step outside of yr soap BOX, just long enough to understand that yr ignorance as a scientist is what lays at the heart of this disease remaining untreated.
fly
>@fly, what does ASD have to do with this? The only people claiming a link between ASD and XMRV et al are truly quacks. I suppose they suggest giving children ARVs as if they are candy. That is sick.
>Anon 8:54 AM,
What is sick is that the epidemiologists who work for our so-called Center For Disease Control, are still ignoring the obvious association between CFS and autism, that proves the infectious nature of the disease. Rather our government seems to be doing their damnedest not to look at it, so we 'quacks' are looking at it. Our informal survey shows us that the incidence of ASD in offspring and siblings of CFS women is much higher than in the general population. Also, partners develop CFS, and related disorders, at a much higher than predicted rate. We are applying for an IRB for a formal survey, with controls, that we intend to publish.
Jamie
>"@fly, what does ASD have to do with this? The only people claiming a link between ASD and XMRV et al are truly quacks. I suppose they suggest giving children ARVs as if they are candy. That is sick."
What Dr Jamie said!