
An important new paper has been published: Xenotropic MLV envelope proteins induce tumor cells to secrete factors that promote the formation of immature blood vessels. Muegai et al. The et al includes Pathak who published the paper with Coffin which identified XMRV as a virus created in the lab. From the title you might think it is about cancer and blood vessels; however, look at the last sentence of the conclusion:
… the results suggest that xenograft approaches commonly used in the study of human cancer promote the evolution of novel retroviruses with pathogenic properties.
Here is the crux of the matter:
The evidence that XMRV was generated as a consequence of studies aimed at elucidating the pathology of human disease is disturbing in that it highlights long feared dangers of use of xenograft tissues in clinical settings, including porcine valves [14,15]. Of even greater concern, the results support the idea that attempts to develop better therapeutic interventions might inadvertently promote the development of pathogenic viruses. However, the following observations refute this possibility: First, although xenotropic and polytropic MLVs have been described as far back as 1970 [16,17], as of yet there has been no validated evidence of human infection by this class of viruses. Second, despite intensive investigation of XMRV by many laboratories [1,18,19] there is no evidence that XMRV is capable of inducing transformation of cells [1,20], although there is recent evidence showing that XMRV infection of LNCaP cells resulted in modest increases in proliferation, and invasion of cells into Matrigel in vitro (Pandhare-Dash et al. [4,21]).
Are you reassured? Their first point is a basic logical fallacy. Absence of proof is not proof of absence. Nobody ever found it, so it isn’t there. Their second point says XMRV, the manmade gamma retrovirus about which we know the most, isn’t dangerous, maybe. What a relief. Yet even they are now admitting, XMRV is not the only one out there. They found a new one for this paper. So now there are at least two, and no longer such a remote possibility.
The studies described herein address these questions, and show that at least one other XMRV-like virus exists, and that the virus evolved the ability to infect human cells and to express gene products that impact tumor pathogenesis.
But no need to panic. The folks that brought you this mess, will figure it out one of these decades. Recombinant Origin of the Retrovirus XMRV, now a year old, where they argued that the chances were “vanishingly small” that XMRV wasn’t created in a lab in the mid 90’s, while studiously ignoring the fact that other similar events were in fact quite likely. So they are finally admitting that the chances aren’t so small, since there have been so many chances. Now there are two. Or is it three? This paper, identified a cell line in use at the NCI that produces another infectious XMLV: The Human Lung Adenocarcinoma Cell Line EKVX Produces an Infectious Xenotropic Murine Leukemia Virus.
Inductive logic is forbidden. No connecting the dots allowed. And who can blame them, when it has been recently demonstrated that dot connecting gets you burned at the stake in the scientific community. Have to start with what we know and carefully build step by step, hoping that the pyramid ends with something coherent. God forbid, we should decide that we have learned something new, something so big that a top down approach should be employed. It is so big in fact, it could explain why 133 million of our people and 55% of our children have chronic illnesses in the US, and why 20% of adults in the developed world have an autoimmune disease. ME/CFS is little. It is time for a revolution. It is an emergency. I wrote that same sentence in 2010 and nothing has changed.
How many young people have been felled by ME/CFS since then? I know about one teenager that was treated in 2010 with antiretroviral drugs and recovered. His mother posted on this blog anonymously at one point, but was presumably prevented from going public. Sick for 8 months, better in 6 weeks. Treated for 6 months and remained in remission off treatment, as far as I know. How did that case report not make it into the literature? It is unconscionable. I am sick of hearing about how an N of 1 is irrelevant. An N of 1 is called a case report. If important enough, it leads to a pilot study and then a clinical trial.
This burden of chronic disease in children is our replacement for the 20% that used to die before the age of 5 of infectious diseases. So instead of dead children we have live disabled ones. What is going to happen to all these disabled children? Whether the cause turns out to be an activated HERV, or an exogenous simple animal retrovirus (alpha, beta or gamma), the use of antiretroviral drugs is a logical thing to try. It is unfortunate that the only drugs available to us were developed for a retrovirus that is phylogenetically dissimilar from the simple viruses in question here, but even so, AZT, Viread, and Isentress have had a positive effect on a number of patients with ME/CFS, incomplete and, after a while, not clearly worth it, but there is a noticeable positive response in a percentage of patients, which appears annecdotally to be greater than placebo. That should be a beacon in the fog, not a reason to make the drugs taboo. Dr. Snyderman’s cancer is stable on full HAART. Shame on both the scientific and medical communities for ignoring him.
What would happen if you gave antiretrovirals to children at the time of an autistic regression? I know your government wants you to believe that the astonishing increase in ASD, now acknowledged by CDC at about 2%, is because we got better at diagnosing it. While that is undoubtedly partially true, since it is now a common disease, it is insulting to our intelligence to reassure people on that basis. It is only 2%, so no worries; your individual chances of having an autisitic child are still low. But what are your chances if you have CFS or a first degree relative with CFS, or autism, GWI, Lyme Disease, PANDAS, RRMS? These diseases are running rampant. Certain families bear an incredible burden of illness, including early aggressive reproductive and hematologic cancers. It is frightening, even if you look at only one disease at a time, but as part of a preapocalyptic whole involving the health of the species? Terrifying. Virus, injury, genetics. Many perfect storms.
Whatever happened to vaccines being inappropriate for people with immunological abnormailities? Given that patients with various immunological problems now encompass a very significant proportion of the population, the entire vaccine program needs to be seriously reevaluated. Continuing to give ever increasing immunological challenges to a patient population with seriously declining immunological health, for diseases that are extremely unlikely to cause long term morbidity or mortality, is no longer clinically justifiable in my opinion. It is medically incorrect and unethical at this point to take the current vaccination schedules for civilians and the military at face value, especially in light of the implications from this paper, and the recent acknowledgement that GWI is not in fact limited to the veterans of Desert Storm, but still occurring.
The upcoming FDA meeting will no doubt give mention to many more dangerous treatment options than AIDS drugs. AIDS patients got the best. Lots of very clean drugs to work with that cost billions to develop. There are probably many drugs on the shelf that didn’t work well enough for HIV, but might have activity against the viruses we are dealing with. My guess is antiretrovirals will not even be on the table for discussion.
IT IS STILL HAPPENING. Every single day. New people getting sick that should be treatable. The scientific community should not be allowed to take their own sweet time about this. It is not acceptable in the midst of this pandemic for them to withhold anything clinically relevant, whilst expressly trying to prohibit the off-label use of legal, safe drugs that might help patients who are in dire straights, patients suffering beyond belief, for whom there is no meaningful treatment. But the culture is to “burn at the stake” any scientist that steps out of bounds, as we have already witnessed. Doctors too, for that matter.
Look at the tunnel vision in this paper. It is all about cancer and xenografts. No mention that gamma retroviruses cause neuroimmune diseases in vivo, as well as cancer. No mention that there are aspects of modern biotechnology that could be causing the same or worse problems than the ones described in this paper, notably hybridoma technology. And nothing about vaccines, the sacred cow, which contain foreign DNA and are parenterally introduced, given in ever increasing numbers and combinations to an ever more vulnerable population. Live attenuated vaccines are grown in cultures known to express animal retroviruses, e.g. chick embryo, mouse brain culture, monkey kidney cells. Here is a list of vaccine excipients and culture mediums used for production from Wikipedia. And that’s now. Can you imagine what the technology was like in the 50’s, 60’s and 70’s? Viruses successively passaged through mouse brains, passaged meaning brain sucked up with a big needle and injected into the next mouse, then eventually the resultant sludge was injected into or fed to people. Now we can tell what we are doing and we are still doing it. Chemical Induction of Endogenous Retrovirus Particles from the Vero Cell Line of African Green Monkeys.
The paper under discussion mentions the “plasticity” of these viruses. They recombine and rescue each other. But scientists aren’t allowed to connect the dots, even when obvious, as it should have been a couple of decades ago, since it was known by the 70’s that these viruses were there. Here, written by a couple of the scientists who have recently contributed to the distortion of the true significance of XMRV, telling us in 1995 what they feared, but did nothing about. I have posted it before and try not to repeat myself, but in light of this paper, it deserves to reappear.
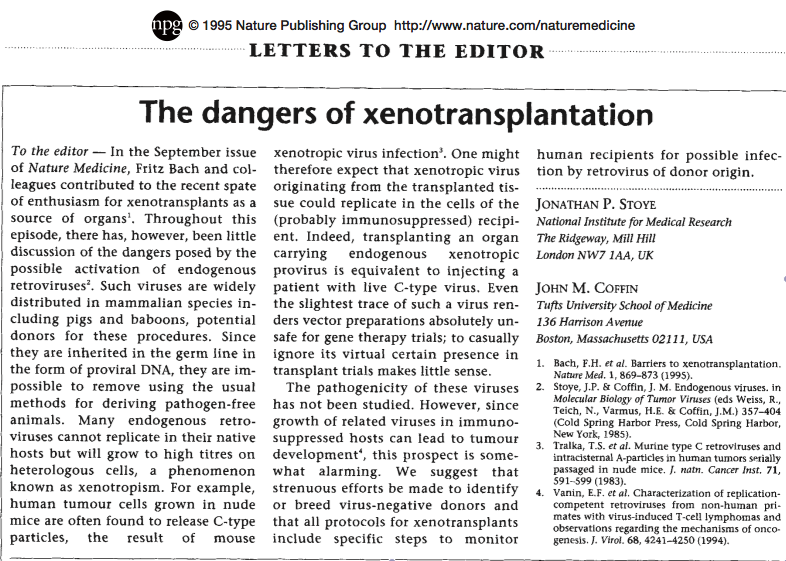
The assumption that these viruses could not harm humans was made on very shakey ground; everybody was having too much fun tinkering to be stopped by a few qualms. There were a few absence of proof experiments. What hubris! Now, this is the only explanation for ALL of the observed phenomena, encompassing the environmental and genetic aspects, the variations on a theme so clear to see in the various patient cohorts. The Lipkin paper came up with positive serology in 6% of the study population, patients and controls, to a very nasty defective murine retrovirus that produces Env. That particular mystery should be a high priority by now. Why is the 6% not being studied intensively? They found positive serology in human beings to pathogenic retroviral Env in Lombardi et al, they found it in Lo et al and they found it in the Lipkin study. The 6% may be, probably is, only one of many. But no need to panic.
On the personal side, as I reported last time, I went back on Viread. I again noticed an uptick in function and ability to withstand stress 6 or 7 weeks after starting it. My blood pressure is now well controlled on additional antihypertensive medicines, in fact better controlled than at any other time in my illness. I started Isentress a couple of days ago and plan to add Kaletra very soon. Ali remains remarkably stable on Viread and Isentress for 3 years now. Her life is very full. She is productive and happy. Her most limiting symptom remains MCS.
I just returned home after a trip to Tucson seeing patients. The first 5 patients I saw were 3 women almost exactly my age and 2 men, both 48 years old and sick for almost four decades. That strikes me as a bit much for coincidence. I have noticed for years, and especially since I’ve been writing this blog, that my December 1953 birth date seems to be at the peak of a bell curve for middle aged ME/CFS women, suggesting something went out horizontally. Was it when we were born? We received the oral polio vaccine, on a sugar cube, but we wouldn’t have all been the same age when we got it, since it wasn’t released until 1961. And we know that there were outbreaks before the polio vaccine. Papers have documented certain years with peak waves of onset. All of this fits with the idea that it has happened multiple times and each time, it looks a little different, e.g. average age of onset, gender susceptibility, most prominent symptoms, thus the misconception that it is a heterogeneous problem.
Just as there were many retroviral invasions in the distant past, in this paper we have emerging evidence that it has happened again, on a grand scale, over a very short period of time. There are most likely already some viruses that are endogenized in families, since it has gone unchecked for so long. The very high incidence of PCOS in young ME/CFS women may be consistent with a retrovirus invading the germline. When I first wrote about this possibility, I thought it was irreparable, a true doomsday scenario, but it is not. Evolution will deal with it, even while our fertility is dropping at an alarming rate. Deletions will occur, possibly in not very many generations. We will learn how to stay methylated to keep our viruses quiescent. We will eventually learn to manipulate epigentic factors in our favor. But like carbon emissions, we need to stop it now. A retrovirus or pieces of a retrovirus now and again, repeated exposures to endocrine disruptors, synthetic hormones and steroids, add a little Bt toxin, a “cover your ass” CT scan and a couple of radioactive tracers for worthless imaging, courtesy of your doctor, and voila! A recipe for the disaster that is occurring, while nobody panics.
Today’s song: You Haven’t Done Nothing by Stevie Wonder
Who got us into the ME/CFS mess. Talk about forbidding inductive logic. There’s no such thing. There’s ME and there’s CFS. ME/CFS is a muddled mess that means whatever anyone wants and different things to different people. Not way to tell how/what patients were selected or what they have. And research results will be meaningless. Some results look good, some look bad. Will not replicate, thus no progress. Sound familiar? Patients play this game at their own peril. We call it out and demand more or nothing will EVER change.
Jill, I understand that this point is near and dear to your heart. I don’t really understand your 2nd and 3rd sentences or what exactly you are implying I have or haven’t done. However, I’ll respond by saying that I think you are incorrect that there exists a distinct patient group that deserves to be called ME and something else that encompasses all waste basket diagnoses of people who aren’t really sick. You are doing to them what has been done to you. The artificial division you are making simply does not exist in the real world. I am evaluating and treating real patients. It is a continuum, not discrete groups. The disease has stages, so some of these people you want to exclude are early stage patients. Any division you can come up with is artificial. Whatever you call it, there are a bunch of symptoms, the order of prominence of those symptoms varies from patient to patient and not everybody has all of them, but the presence or absence of a particular symptom doesn’t make me think a patient has a different disease. I understand why it matters to you as an advocate, but it is clinically meaningless.
I agree completely with you, Jamie.
Jill, I can fit myself into at least 3 categories, no 4. I have Lyme disease, I have CFS, I have ME, and if I want to get some Lyrica I have fibromyalgia. I also have Hashimoto’s and have very bad reactions to mold toxins. So put me in a study and see what turns up. Assuming all of the above are different disease states then once we test for a lot of crap the groups will form naturally. Until we do this we have no clearcut groups. I keep looking for Fallon’s study of spinal fluid proteins that were different in CFS vs Lyme patients. Oh how we need to form these groups and then figure out why the proteins are different.
I think its very brave of dr Pathack to admit that tpathogenic gammaretroviruses generated by experiments with mice are probably replicating and causing pathology in the human population. I agree that they should have stressed that gammaretroviruses cause quite horrendous neurological and autoimmune diseases as well as being oncoviruses. Replication defective gammaretroviruses are particularly pathogenic. The argument posed against the presence of GRVs in the human population is very weak as anyone who understands the principles of PCR will testify to its inability to discover new retroviruses whose sequence is not know. In this case absence of evidence is certainly not evidence of absence.The chances that GRV recombinants are not at large in the Human population is vanishingly small.There are a number of reasons why we find ourselves in this prediciment. CFS is an irrational name for the Incline village disease or ramseys disease yet the world health organisation holds that chronic fatigue syndrome and ME are different names for the same neuroimmune disease. The problem in practice is that very many people diagnosed with ME or CFS or ME/cfs do not have a neuroimmune disease. At the moment no one knows what the biomedical abnormalities which are specific to ME are and ME like CFS is a phenotypical classification. The future lies in establishing a diagnostic test and not simply saying that ME is not CFS. The task would be to construct a scientific definition of ME which does not rely on the twin pillars or phenotype and circular reasoning
Agree completely, Gerwyn.
Medical history throws many curious details.
Yellow fever
“Medical history was made in 1927 when Stokes, Bauer, and Hudson infected rhesus monkeys with blood from Asibi, a native of the Gold Coast (now Ghana) with a mild attack of yellow fever. The Asibi strain proved not to be benign and several deaths in laboratory workers were subsequently attributed to it. Nevertheless, it was the strain of yellow fever virus that between 1933 and 1937 Theiler, Lloyd, Smith and coworkers attenuated by multiple passage in mouse brain and chick embryo tissue.
The human trials of this 17D vaccine certainly showed that the 176 or more passages in non-primate tissues had greatly attenuated it, and once problems due to lability of the vaccine and the mistaken use of pooled human serum as a stabiliser11 were ironed out it was hailed as a triumph. No serious attempt was made thereafter to develop an alternative as the 17D vaccine was regarded as safe and effective for at least 10 years, and infancy, pregnancy, egg allergy, and immunosuppression are its only present contraindications.”
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1122380/
Yellow fever
“Between the 89th and 114th in vitro passage (from the start of the experiment, that is including the passages in embryonic mouse tissue and whole chicken embryos) a marked change in virulence of the virus occurred. The reason for the change in virulence is unknown and attempts to repeat these experiments by virus s passage have failed to develop additional avirulent strains. The 17D strain has been widely used as a human vaccine, being safe and highly effective.”
http://www.pnas.org/content/84/7/2019.full.pdf
Polio
Successful Transfer of the Lansing Strain of Poliomyelitis Virus from the Cotton Rat to the White Mouse
http://www.jstor.org/discover/10.2307/4583135?uid=3738032&uid=2&uid=4&sid=21101861999151
Polio
“Also working at Lederle was Polish-born virologist and immunologist Hilary Koprowski, who claims to have created the first successful polio vaccine, in 1950.
Koprowski’s attenuated vaccine was prepared by successive passages through the brains of Swiss albino mice.
On February 27, 1950, Koprowski’s live, attenuated vaccine was tested for the first time on an 8-year-old boy living at Letchworth Village, an institution for the physically and mentally disabled located in New York. After the child suffered no side effects, Koprowski enlarged his experiment to include 19 other children.”
http://en.wikipedia.org/wiki/Polio_vaccine
WHO 1952 – Yellow fever
“The use of mouse brain virus seems”, according to Smithburn, “to be a more objectionable feature. There is always the possibility that the yellow-fever virus may become contaminated with another virus that the mouse may be harbouring… Lastly, there is also the potential hazard, whenever mammalian tissue is employed in a vaccine, of allergic demyelinating encephalomyelitis.”
http://apps.who.int/iris/bitstream/10665/75301/1/WHO_YF_20_eng.pdf
Many papers about infected cell lines.
Detection of murine leukemia virus in the Epstein-Barr virus-positive human B-cell line JY, using a computational RNA-Seq-based exogenous agent detection pipeline, PARSES.
” Finally, reverse transcription-PCR analysis showed the presence of MuLV in three other human B-cell lines (DG75, Ramos, and P3HR1 Cl.13) commonly used by investigators in the Epstein-Barr virus field. ”
http://www.ncbi.nlm.nih.gov/pubmed/22238296
Infection of human cells by an endogenous retrovirus of pigs.
http://www.ncbi.nlm.nih.gov/pubmed/9055854
Thank you Jamie, still coming to terms with the news I received yesterday that I am Lyme posative.
Thanks for this article Dr. Jamie !
I hope no one minds my tangent: you say ” 20% of adults in the developed world have an autoimmune disease”. I take it you also have the impression that people in developed or industrialized countries are more likely to get ME/CFS than people in
less developed countries ?
From my travels and communications I have the impression that people in developed, advanced countries get ME/CFS more often.
Does anyone have any thoughts on why this might be the case ?
Thank you for this passionate & informative post, Jamie.
You mentioned the relative ages of your patients – I will be 50 in June (born in 1963) and have noticed that off my legion of ME/CFS friends, very many are within 3 years of my age, and a striking number within a year. I participated in the informal family study you did, and am curious if you came across any particular ages (or years of birth) that had spikes in the incidence of ME/CFS? It seems clear we all got “something” the same…
Thank you!
Interesting the xenotransplantation paper came out in 1995. Also in 1995, the biosafety level changed for MLV’s from a safety level 1 to safety level 2. It was done by Harold Varmus: http://www.gpo.gov/fdsys/pkg/FR-1996-01-19/html/96-689.htm Then in 1999 CFS was moved out of NIAID and into Office of Research on Women’s Health. This is where ME/CFS has been for decades with little to no funding for research. Now the reason I have an interest in all this is because I, and most of my immediate family members have the misfortune of being sick with various neuroimmune diseases, vasculitis, and cancers. Interesting given this new paper just out!. These illnesses include Parkinson’s, MS, Breast Cancer/ischemic colitis/mild stroke, Graves disease/heart attack age 44, 2 cases of ME/CFS/Fibromyalgia, and my oldest brother died from Leukemia. Only one brother is healthy and he recently started suffering from chronic migraines. So yes this part from above is interesting given my family history: ” Look at the tunnel vision in this paper. It is all about cancer and xenografts. “No mention that gamma retroviruses cause neuroimmune diseases in vivo, as well as cancer.”
And yes I find this conclusion from the new Panthak paper quite interesting as well: “the results suggest that xenograft approaches commonly used in the study of human cancer promote the evolution of novel retroviruses with pathogenic properties.”
Great song choice too Jamie, I Love Stevie!
I am not however happy about what’s happened to my family! And mine is not the only one.
I really dont see how anyone can expect science to provide any answers about the cause of Incline village or Ramsey’s disease unless science is involved in selecting patients to be studied. In practice the CFS label is attached to people who have primary depression, somatoform disorder stress induced immunodeficiency syndrome,burnout, personality disorders as well as those having Incline Village disease.In my view no one should have been entered into the so called lipkin study without a record being made of their underlying cytokine profiles Th2 Th1 biases and so on.There are certain cytokine profiles which are characteristic of a retrovirus infection in general and a gammaretrovirus infection in particular.Thus if a scientist were to construct a study searching for the presence of a gammaretrovirus then he or she would select patients for that study which had the highest likelihood of carrying gammaretroviruses. This was simply not done in the Lipkin study. A scientist would also know that gammaretrovirus families tend to consist of replication defective pathogens and one or more helper viruses and thus have a PCR setup capable of detecting sequence variants.This was not done in the lipkin study. Thus when Pathack says that there is no evidence of a family of gammaretroviruses at large in the human population although there is a strong likelyhood that there are that is hardly surprising as their approaches have lacked the flexibility to detect them. The people who supplied the patients to the lipkin study continually produce studies recruiting patients whose immune profiles have all the characteristics of stress induced immunodeficiency syndrome and cite epstein barr as a putative cause. Once again establishing cause and effect becomes impossible as immunosuppression itself leads to the activation of Herpes viruses.One cannot diagnose based on symptoms. That would usually lead to an action in negligence if the diagnosis was later found to be incorrect.Can anyone imagine a trial looking for a viral cause of MS without establishing that people in the study actually had MS and not just fatigue and a few minor symptoms of idiopathic or psychological origin.The Scientific community would laugh at such a study design yet the lipkin study with exactly the same design is lauded. Dr Lipkin said that the patients he investigated who purportedly suffered from Incline Village disease in the past had evidence of polyclonal B cell proliferation.Why in heavens name didn’t he insist on recruiting patients displaying that abnormality? Polyclonal ( and later oligoclonal) B cell proliferation is vitually diagnostic of a gammaretroviral infection. The conclusions and design of the Lipkin study are, from a scientific perspective,wholly unsound
Could vaccines cause a neuroimmune disease in children?Yes they could in theory via number of different mechanisms.Multiple vaccines are in reality a huge immune insult which can cause prolonged activation of the immune system lasting for many months.This can in turn lead to the activation of a number of self sustaining inflammatory pathways leading to chronic activation of glial cells in the brain resulting in severe neuropathology.Alternatively infectious agents could be introduced by highly suspect and cavalier manufacturing processes involving the passage of viruses through cell lines which are essentially of primate or murine origin.Some live vaccines are created using viruses which have undergone attenuation by literally hundreds of passages through cell lines or cultures derived from mouse brains !!! I must emphasize that I am not against vaccination per se which I believe to be an essential method of creating and maintaining herd immunity. The practice of giving multiple or single vaccines to young children,however, without checking for underlying immune abnormalities first is simply inviting disaster. In all honesty we cannot yet answer the question as to whether vaccines cause neuroimmune pathology in children or adults or not. The problem lies once again in phenotypical classification.We are invited to believe that everyone displaying the triad of abnormalities which lead to the classification of autism have the same disease processes leading to that symptom profile ( This is quite apart from ignoring the plethora of symptoms and biomedical abnormalities detected in many children carrying the diagnosis of autism) This of course is the mickey mouse school of medicine !! If scientists are serious in answering the question of whether or not vaccines cause neuroimmune disease in children then they would select children with overt neuroimmune abnormalities which carry a diagnosis of autism and not select on the basis of symptoms which could have a myriad of different causes. Is it really too much to expect the rigorous application of the scientific method and scientific reasoning while attempting to answer such a fundamentally crucial question
14 months on bio-identical Estriol 20 mg/Progesterone 50 mg , with every month continuing to bring improvements. This was mentioned in a comment on this blog.
Do take many supplements, including ribose = key to hypothalamus function.
A German MD doing clinical research in the USA (links below) has documented that WiFi ( pulsed microwave radiation) splinters both the genome, and the mature DNA / mitochondria . And that WiFi induces , in severity directly proportional to exposure , all of the spiking organism failures like MS, Autism, Parkinsons, Alzheimers, Diabetes Type 3 , Lupus, ME…AD INFINITUM.
http://www.youtube.com/watch?v=b_wxM6IAF1I
http://www.klinghardtacademy.com/Videos/
“But no need to panic. The folks that brought you this mess, will figure it out one of these decades. Recombinant Origin of the Retrovirus XMRV, now a year old, where they argued that the chances were “vanishingly small” that XMRV wasn’t created in a lab in the mid 90′s, while studiously ignoring the fact that other similar events were in fact quite likely. So they are finally admitting that the chances aren’t so small, since there have been so many chances. Now there are two. Or is it three?”
Jamie, will you please at least get the above correct? When you make such fundamental errors it really detracts from the rest of your argument since it makes it look like you have absolutely no grasp of what is being discussed. The “vanishingly small” chances referred to in the ‘Recombinant Origin of the Retrovirus XMRV’ paper have absolutely nothing whatsoever to do with there being a ‘vanishingly small’ chance of XMRV itself being produced, or even any number of XMRV-like/type viruses being produced. The ‘vanishingly small’ reference is in regards to there being a ‘vanishingly small’ chance that a virus which was 100% identical to XMRV being produced twice in seperate recombination events. This led the authors to conclude that since the chances were so ‘vanishingly small’ for an identical (not similar, not related, but 100% identical) retrovirus to be produced twice in independent recombination events, it was indeed the case that the virus known as XMRV was produced in the manner in which they described in the paper and not produced once in a lab rat and once again in another seperate and completely unrelated event, ie ‘out in the wild’.
I’ve tried explaining this before, but ‘vanishingly small’ has absolutely nothing whatsover to do with any number of recombinant retroviruses being produced in the manner in which you hypothesize, but rather has to do with the potential for two (or more) 100% identical recombinant retroviruses being produced in seperate and unrelated recombination events. You and others are and have been completely misinterpreting what was said for quite some time and it makes you look foolish to keep doing so.
Please reread this sentence?
” they argued that the chances were “vanishingly small” that XMRV wasn’t created in a lab in the mid 90′s, while studiously ignoring the fact that other similar events were in fact quite likely.”
You have missed the point, John. Focusing only on XMRV, while ignoring the broader implications, is a form of obfuscation.
That’s because the paper you cite was on the origin of XMRV, hence the title ‘Recombinant Origin of the Retrovirus XMRV’. Please re-read this sentence- “So they are finally admitting that the chances aren’t so small, since there have been so many chances. Now there are two. Or is it three?” I thought you might have understood but your statements contradict themselves. They never said the chances of similar recombinant retroviruses occuring were small to begin with, did they? Any given paper cannot touch on every single aspect of a given situation, it can only deal with the topic that the paper was written to deal with. As the current paper shows, the authors are not ignoring the broader implications, they’re simply describing what has been shown by their work and are in fact actively working to broaden the research base on the subject.
I don’t have a problem with your basic argument, I’ve just seen the ‘vanishingly small’ thing repeated fairly recently (oddly enough by someone who also was a big bugaboo during the whole XMRV fiasco and who would spin scary tales to the chirruns by the campfire) and wanted to clarify the subject.
This is the actual quote from the Paprokta paper.
“Because the probability that the same recombination event could occur independently by random chance is essentially negligible, any XMRV isolates with the same or nearly the same sequences identified elsewhere originated from this event ”
The other way of looking at this concusion is that it was the product of the authors belief that XMRV was created by these recombinant events. The chances of that actually being true in the first place had the same odds as having it happen again, i.e. vanishingly small.
And as I pointed out they failed to demonstrate that their quantitative PCR could detect XMRV nucleic acid below a concentration of 2000 copies per 100 cells.
So the results are open to interpretation. One can either conclude that the results were a product of an unvalidated PCR of unknown clinical sensitivity which could not detect GRV DNA in early xenografts, or, evidence of an astronomically unlikely series of recombination events.
This is what I’m talking about- when you say that “The chances of that actually being true in the first place had the same odds as having it happen again, i.e. vanishingly small”, this is completely incorrect and shows your lack of even the most basic understanding of the subject. For a given recombination event to occur once is no big deal, however for the exact same recombination event to happen twice is vanishingly small, which is why the authors write “Because the probability that the same recombination event could occur independently by random chance is essentially negligible…”. Think of it like two individuals having a child together- it’s really not that uncommon. But the chances of the same individuals having the exact same child twice as a result of seperate fertilization events are vanishingly small, even though all of the same genes are present.
Actually that it not correct and they failed to demonstrate that their quantitative PCR could detect XMRV nucleic acid below a concentration of 2000 copies per 100 cells. From that point any conclusion the authors made is purely speculation.
Dr Mikovits told us 4 years ago its not XMRV it’s XMRVsssssss
XMRV is the name given to 1 sequence. Other gamma retroviruses are not XMRV. Which means there is evidence for other gamma retroviruses in ME, not THE sequence they call XMRV.
Jamie, I have been ruminating over the sugar cube polio live vaccine I got. I am 67 and got the polio shot around 1955. Then in January, 1957 we moved to Philadelphia. While I attended a private grade school there I was given the sugar cube. That had to have been no later than the spring of 1959. A local doctor who had a daughter in our school came in and gave all of us that sugar cube which does not seem to have been on the market yet. I wonder if that doc was part of a clinical trial group related to Kaprosky at the Wistar Institute? I can’t see how else I got that live vaccine. Of course, I have to add that I have no clue if this has any relevance to my developing CFS many years later at the age of 50. I just find it curious.
Dear Jamie,
I have no other way to publish this. I am no longer on forums, nor FB or any other social forum, because I have been hacked and cyber stalked for month – I am to sick to take such crap -, but I continue to study, and what I found is important and will interest you very much. So excuse me if I use this avenue to get the word out.
FRIENDS – an old friend is manipulating the immune system
Immune Markers
Several important studies on immunological abnormalities in patients diagnosed with ME/CFS have been published: two studies from Australia (Brenu et al.), China (LIU Ding-hua) and now another study from Spain.
About six month ago I showed the papers from Brenu et al. to a cancer doctor and asked her what she is thinking about it? She took one look at it and commented ” similar immune markers are found in many cancers”.
I was surprised.
One thing led to the next and I found myself studying cancer-immune research.
I started out with cancer research and ended up with infectious diseases. A pretty amazing journey and if you bear with me I am sure you will find this write up an eye opener. I am not a scientist nor doctor and I am sure there are others in our community including our specialists better qualified to talk on this topic in detail, but it seems to me nobody is talking about it. WHY?
I will try to summarize what I found and learned (quote a few texts to make it easier for me) and attach a some interesting studies which I think are relevant.
Lets back track a bit and just compare what three studies found.
The study by Brenu et al. found an increase in IL-10, IFN-Y, TNF-a, CD4+CD25+T cells (Treg) FoxP3, Perforin, VPACR2 expression and a decrease in CD8+T
Cells, NK cells phenotypes CD56 bright in patients diagnosed with ME. http://www.translational-medicine.com/content/9/1/81
The Chinese study China (LIU Ding-hua): “The results showed that the NK cells, CD4+T cells and CD25+ regulative T cells in CFS patients were higher and B cells were lower than that of healthy controls, while there was no significant difference between CFS patients and healthy controls with respect to the percentage of T cells and CD8+T cells and CD4+/CD8+ ratio”http://www.meassociation.org.uk/?p=10436
And the Spanish study found: “CFS diagnosed individuals showed similar absolute numbers of T, B and NK cells, with minor differences in the percentage of CD4+ and CD8+ T cells. B cells showed similar subset frequencies and proliferative responses between groups. Conversely, significant differences were observed in T cell subsets. CFS individuals showed increased levels of T regulatory cells (CD25+/FOXP3+) CD4 T cells, and lower proliferative responses in vitro and in vivo. Moreover, CD8 T cells from the CFS group showed significantly lower activation and frequency of effector memory cells. No clear signs of T-cell immunosenescence were observed. NK cells from CFS individuals displayed higher expression of NKp46 and CD69, but lower expression of CD25 in all NK subsets defined. Overall, T cell and NK cell features clearly clustered CFS individuals. http://www.ncbi.nlm.nih.gov/pubmed/23514202
If you compare all three studies there are differences in their finding’s and some results seem to contradict each other or are just to complex to discuss here in details, especially as a layman patient, but there is some remarkable overlap in all three studies which must change how you, and the science community, views ME/CFS.
All three studies have found a significant increase of Tregs!
The Chinese study (LIU Ding-hua): ” CD4+T cells and CD25+ regulative T cells in CFS patients were higher …..”
The study by Brenu et al. found:” an increase in IL-10 IFN-Y, TNF-a, CD4+CD25+T cells (Treg) FoxP3”
The Spanish study “A key factor in the control of T cell responses is the function of Treg cells, which are significantly increased in our cohort of CFS individuals confirming data from another recent study .”
In order to understand the significance of this findings one has to acquire some basic knowledge about immune markers.
Mini crash course in immunology – as I understood it
T cell is a lymphocyte of a type produced or processed by the thymus gland and actively participating in the immune response. Also called T lymphocyte.
B cells are a lymphocytes not processed by the thymus gland, and responsible for producing antibodies.
”There are two main types of T-cells. T-4 cells, also called CD4, are “helper” cells. They lead the attack against infections. T-8 cells (CD8) are “suppressor” cells that end the immune response. CD8 cells can also be “killer” that kill cancer cells and cells infected with a virus. Researchers can tell these cells apart by specific proteins on the cell surface. A T-4 cell is a T cell with CD4 molecules on its surface. This type of T-cell is also called “CD4 positive,” or CD4.”
The CD system is used as cell markers in immunophenotyping and they are usually grouped, called cluster of differentiation (cluster of designation), associated with certain immune functions. Cluster of differentiation can aid in a diagnosis and monitor disease progression/regression in clinical trials. For example in cancer they are used to monitor the effectiveness of therapies, or the progression of cancer. Another marker well known is the CD4 marker in HIV – CD4 and CD8 cells are used to monitor the progression in HIV infection.
http://en.wikipedia.org/wiki/Cluster_of_differentiation
“In humans, Treg represent 10% of circulating CD4+ T cells. They are defined functionally by their capability to suppress the activation and proliferation of CD4+ and CD8+ effector T cells (effector cell acts in response to a stimulus). But regulatory T cells (T-reg) that control harmful autoimmune T cells in the periphery may also suppress the immune response against cancer.”
“Forkhead box P3 (FOXP3) – expressing regulatory T cells (Treg) have a pivotal role in the regulation of immune responses.”
(There are various subgroups of Tregs and a complicated interaction between Tregs and T effector cells (and other cells) determine the immune response – a topic which deserves a separate discussinon)
“Naturally occurring thymus-derived CD4+CD25+ regulatory T-cells (Tregs) play a critical role in the control of immune responses in various clinical settings, including autoimmune diseases, allergic disorders, infections, transplantations, and cancers.”
“In humans, an increase in CD4+CD25+ T cell numbers has been detected in the blood of patients with cancers of diverse nature, including oesophageal and gastric, colon, pancreas and breast, melanomas, hepatocarcinoma, cervical and endometrial , ovarian and lung carcinoma and Hodgkin’s disease. CD4+CD25+ T cells may also accumulate within the tumor site or at its vicinity and in the draining lymph nodes. The percentage of Treg cells among peripheral blood T cells was shown to correlate with prognosis.”
Alteration in the number and function of Tregs has also been implicated in several autoimmune diseases, including MS, RA and type 1 Diabetes. But Tregs in autoimmune disease are usually decreased, exempt in virus induced autoimmune models, and upregulation is considered to prevent autoimmunity. The ability of various therapies to regulate the differentiation and function of Treg cells in autoimmune or allergic diseases has been the subject of many recent studies. It deserves a separate write up, but here a few excerpts.
“In adjuvant-induced animal models of autoimmune disease, depletion of regulatory T cells increases inflammation while administering these cells can reduce or even prevent disease. Thus, the balance between effector T cells and regulatory T cells may determine whether autoimmune disease develops or…”
“Collectively, our findings indicate that susceptibility to a virus-induced autoimmune disease can be regulated by differential responses of Tregs to the infectious agent which may be an important factor in regulating genetic susceptibility to various human autoimmune diseases.”
“(TMEV-IDD) serves as virus-induced model of chronic progressive multiple sclerosis. Infection of susceptible SJL/J mice leads to life-long CNS virus persistence and a progressive autoimmune demyelinating disease mediated by myelin-specific T cells activated via epitope spreading. In contrast, virus is rapidly cleared by a robust CTL response in TMEV-IDD-resistant C57BL/6 mice. We investigated whether differential induction of regulatory T cells (Tregs) controls susceptibility to TMEV-IDD. Infection of disease-susceptible SJL/J, but not B6 mice, leads to rapid activation and expansion of Tregs resulting in an unfavorable CNS ratio of Treg: T effector cells. In addition, anti-CD25- induced inactivation of Tregs in susceptible SJL/J, but not resistant B6, mice results in significantly decreased clinical disease concomitant with enhanced anti-viral CD4+, CD8+ and antibody responses resulting in decreased CNS viral titers. This is the first demonstration that virus-induced Treg activation regulates susceptibility to autoimmune disease differentially in susceptible and resistant strains of mice and provides a new mechanistic explanation for the etiology of infection-induced autoimmunity.” http://www.ncbi.nlm.nih.gov/pubmed/21273044
FRIENDS – an old friend is manipulating the immune system
Interestingly, regulatory T-cell activity has also been reported to increase in several infectious contexts, such as retro-viral infections, mycobacterial infections, various parasitic infections including Leishmania and Malaria.
“Tregs have been shown to be detrimental to viral clearance mechanisms in several chronic viral infections including hepatitis C virus, herpes simplex virus, Friend leukemia virus and, most recently, human immunodeficiency virus”
“Current hypotheses suggest that upon encounter with infectious microorganisms, the activity of regulatory T cells may be down regulated, either directly or indirectly, by other cells to facilitate elimination of the infection. Experimental evidence from mouse models suggests that some pathogens may have evolved to manipulate regulatory T cells to immune suppress the host and so potentiate their own survival.” http://www.immunehealthscience.com/immune-system.html
Various studies explain the mechanism by which (FV) viruses seem to manipulate Tregs, cause CD8+ T cell disfunction and impair virus clearance causing chronic low grade infections. If I understood this correctly, a mechanism which does not only fit into the findings of a low CD8+ activity in two studies (Spanish/Australien Study), but it fits the pathology of ME/CFS like a glove.
“Contemporaneous with the development of CD8+ T cell dysfunction, different CD4+ T cell populations expressing cellsurface markers for Treg and the Treg-associated transcription factor Foxp3 expanded. Transfer as well as depletion experiments indicated that regulatory CD4+ cells developed during the second week of FV infection and subsequently suppressed CD8+ T cell functions, which was associated with impaired virus clearance.” http://onlinelibrary.wiley.com/doi/10.1002/eji.200636059/full
“To this end we have studied mice chronically infected with Friend retrovirus. These studies have revealed a mechanism of escape and maintenance of persistence that appears to be common among chronic infections of many types including viral, bacterial, parasitic and fungal infections. Either by direct or indirect means, chronic infectious agents are able to subvert the regulatory T cell system that normally prevents autoimmune diseases and immunopathology. Studies of mice chronically infected with Friend virus have revealed a complex balance of immune responses including two distinct CD4+ T cells subsets with opposing effects. A CD4+ T cell effector subset exerts the antiviral activity required to keep virus replication in check while a CD4+ regulatory subset suppresses the ability of CD8+ T cells to eliminate the infection.”
“As mentioned, the finding that depletion of CD8+T cells had no effect on chronic virus suggested that the virus had escaped control by these important immunological effectors. Investigation into possible escape mechanisms such as virus latency, CTL epitope mutation, and interference of antigen presentation revealed that FV was utilizing a novel mechanism of escape. First of all, quantitative PCR experiments revealed that the virus was not latent. Although the percentage of infected cells was extremely low compared to acute infections, virus transcription on a per-provirus level was equivalent.” http://www.frontbiosci.org/2007/v12/af/2167/fulltext.htm
These results demonstrate the important role of Treg in controlling acute retrovirus-specific CD8 T-cell responses, and suggest that temporary manipulation of Treg might be a possible therapeutic approach in chronic infectious diseases. http://bloodjournal.hematologylibrary.org/content/114/15/3199.full.pdf
“In acute, self-limited virus infections, a vigorous CD8 T-cell response leads to viral clearance. However, many viruses induce persistent infections, despite continuous measurable CD8 T-cell responses (103), a situation in which Treg may be involved. Although Treg activity could be beneficial to the host due to a suppression of tissue damage mediated by virus-specific effector T cells, those T cells simultaneously inhibit the host immunity important for viral clearance and thus may contribute to persistent infection.
Some might remember the long term study done in Australia on patients infected with Q. Fever. Here is an article which talks about Tregs being up regulated in Chronic Q Fever: ”Tregs may be critical for the chronic evolution of Q fever”
“Chronic Q fever, which principally manifests as endocarditis, is characterized by Coxiella burnetii persistence and an impaired cell-mediated immune response. The long-term persistence of pathogens has been associated with the expansion of regulatory T cells (Tregs), the CD4+ T-cell subset that is characterized by the expression of CD25 and Foxp3. We investigated the presence of Tregs in patients with acute Q fever (n = 17), known to exhibit an efficient immune response, patients with Q fever endocarditis (n = 54) and controls (n = 27) by flow cytometry. The proportion of CD3+, CD4+ and CD8+ T cells was similar in controls and patients with Q fever. The percentage of CD4+ T cells that expressed CD25 was similar in controls and patients with Q fever. The population of CD4+ T cells that expressed both CD25 and Foxp3 was significantly (P < 0.001) increased in patients with Q fever endocarditis compared with controls. Our data suggest that the expansion of Tregs may be critical for the chronic evolution of Q fever.”
Yasmine Belkaid&Barry T Rouse’s review put the nail in the coffin for ME – so to speak. They discuss the control exerted by natural CD4+CD25+ regulatory T cells during infectious process.
Here just a view excerpts of this review
“Reactivation of latent or chronic bacterial (for example, Mycobacterium tuberculosis), protozoa (for example, Leishmania sp. or toxoplasma) and viral (for example , herpes viruses) infection an immense burden of morbidity and mortality. Reactivation can occur as a result of immunosuppression or environmental insults or with advancing age, but a definite cause for the reactivation or primary activation of dormant infection is often not apparent. In some situations, increased Treg cells can lead to disease reactivation. In the mouse model of chronic leishmania infection, for example, the transfer of purified natural Treg cells derived from infected mice into other chronically infected animals is sufficient to trigger disease reactivation and inhibit effector memory response. Further more, secondary challenge of mice chronically infected with leishmania at a site distant from the initial infection site induces transient disease reactivation at the primary inoculation site despite induction of a powerful immune response at the challenge site. Reactivation is associated with a local increase in the number of natural Treg cells. There results demonstrate that the equilibrium between natural Treg cells and effector lymphocytes can disturbed by super infection, thereby altering immune efficacy and disease reactivation.”
“We also have found natural Treg cells among the inflammatory cells in HSV-infected sensory ganglia. Here we believe hat natural Treg cells may serve to prevent effector T cells from destroying the infected but irreplaceable neurons.”
“ In conclusion, natural Treg cells participate in the immune response to many and perhaps all infectious agent. Usually they serve to restrain exuberant immune reactivity, which in many chronic infection benefits the host by limiting tissue damage. However, the natural Treg cell response may handicap the efficacy of the protective immunity, includineg that induced by vaccines. …..”
http://www.nature.com/natureimmunology
Last but not least: “Treg can also suppress the function of B cells, NKT cells, NK cells and DC, in addition to T cells” http://jvi.asm.org/content/82/1/21
Summary
High Tregs are markers all three studies can agree on. Regulatory T cells play an important role in maintaining immune homeostasis. High levels of Tregs have been found in many cancers and various viral context. High Tregs are known to cause immune suppression and could explain many of the other immune abnormalities, and thus explain the inability to clear chronic infections.
I am saying it with more conviction than ever, immune markers are the key to validate and possible explain a disease misleadingly named and classified as ME/CFS, which should be named and classified as an “acquired chronic immune disfunction of unknown etiology”
I hope I could convey to everyone the significance of these immune markers.
A personal note
We all agree that CFS is nothing else than a convenient waste bucket classification, with severe consequences for us patients. In my view the diagnosis of ME as primary neurological is also questionable, especially considering those immune abnormalities and the history of ME.
Here a well researched and discussed in an article by E.D. Acheson, “ The clinical Syndrome Variously Called Benign Myalgic Encephalomyelitis, Iceland Disease and Epidemic Neuromysthenia” a , http://www.sciencedirect.com/science/journal/00029343
NKcells and Rituximab
That NK cells activity is “skewed” in ME/CFS patients is no news and many are familiar with the topic. But NK cells consist of subgroups and add to the complexity of the immune disfunction in various immune diseases. Cancer research has gained new insights into their functions and purpose in normal immune surveillance of NK cells, and developed therapies to eliminate tumor cells through monoclonal antibodies like Rituximab – a topic which should be of interest to us.
Here a some interesting excerpts:
“Since their discovery more than 3 decades ago, our knowledge about the function of human NK cells has grown exponentially. Once considered a forerunner of the seemingly more sophisticated antigen-specific, memory-bearing adaptive immune system, it is now clear that NK cells are highly sophisticated players of the innate immune system with certain recognition features that arrived on the evolutionary scene with primates approximately 400 million years after the birth of adaptive immunity.”
“During the past 2 decades there has been a substantial gain in our understanding of what and how NK-cells “see,” lending important insights into their functions and purpose in normal immune surveillance. The most recent discoveries in NK-cell receptor biology have fueled translational research that has led to remarkable results in treating human malignancy.” http://www.ncbi.nlm.nih.gov/pubmed/18650461
”Natural killer (NK) cells have been the focus of interest of immunologists for almost two decades. The increasing knowledge of NK cell biology acquired throughout this period has led to a paradigm shift – for a long time NKcells were considered merely as relatively primitive killers but they are now seen not only as bona fide actors in innate immunity but also as important cells that shape and influence adaptive
immune responses and are more and more being endorsed with an immune regulatory role. However, NK cells are not a homogeneous cell population and several subtypes exist in both human and mouse.” http://www.ncbi.nlm.nih.gov/pubmed/19278419
A paper from Germany by Rauf Bhat and Carsten Watzl describes how NKcells undergoes functional exhaustion: “NK cells undergo functional anergy or exhaustion after carrying out their killing action. Previous studies have demonstrated that after an exposure to target cells, NK cells undergo inactivation, lose their cytotoxic function and become apoptotic. Cytotoxicity of NK cells is executed mainly through the granule exocytosis pathway where Perforin and Granzyme B content of granules is released into the immunological synapse after conjugate formation with targets. This results in a depletion of these components and in a loss of cytotoxicity. Whether the cytotoxic function and granular content of NK cells, which have already participated in serial killing and have undergone inactivation can be reversed is still unknown.”http://www.plosone.org/article/info:doi/10.1371/journal.pone.0000326
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1828617/
A much discussed topic in cancer research"Anti-cancer therapies utilizing monoclonal antibodies also rely on the cytotoxicity of NK cells for their effectiveness.”
“Natural killer (NK) cells are powerful effectors cells that can be directed to eliminate tumor cells through tumor-targeted monoclonal antibodies (mAbs). Some tumor-targeted mAbs have been successfully applied in the clinic and are included in the standard of care for certain malignancies. Strategies to augment the anti-tumor response by NK cells have led to an increased understanding of how to improve their effectors responses. Next-generation reagents, such as molecularly modified mAbs and mAb cytokine fusion proteins (immunocytokines, ICs) designed to augment NK-mediated killing, are showing promise in preclinical and some clinical settings. Continued research into the anti-tumor effects induced by NK cells and tumor-targeted mAbs suggests that additional intrinsic and extrinsic factors may influence the anti-tumor response. Therefore more research is needed that focuses on evaluating which NK cell and tumor criteria are best predictive of a clinical response and which combination immunotherapy regimens to pursue for distinct clinical settings.” http://www.ncbi.nlm.nih.gov/pubmed/21660134
http://www.hindawi.com/journals/biomed/2011/379123/
Jamie
You might find this interesting
http://multiple-sclerosis-research.blogspot.co.uk/2013/05/raltegravir-in-ms-recruitment-update.html
https://www.ncbi.nlm.nih.gov/pubmed/23656710