My muse left on extended vacation when the Lipkin XMRV study and subsequent press conference succeeded in discrediting retroviruses as a possible explanation for ME/CFS, with lots of important questions still left unanswered. The discussion reverted to whether or not it is a real disease and which set of diagnostic criteria are best, so there hasn’t been much to inspire me. It got pretty depressing. The IOM report was a joke: “The term ‘myalgic encephalomyelitis’ is not appropriate because there is a lack of evidence for encephalomyelitis (brain inflammation) in patients with this disease…”. Fail. I don’t know what to make of the Lipkin cytokine paper, because I take with a grain of salt results from a debunker on call for the government. XMRV wasn’t the first time: Lack of association between measles virus vaccine and autism with enteropathy: a case-control study. Nothing worth blogging about there. Certainly nothing hopeful. But recently, the Naviaux study was published and a couple of proposals posted by NIH have been making the rounds on Facebook, so I’ve had an uptick in email, some asking what I think about the paper and some telling me about successes with antiretrovirals in Europe, as well as encouragement to blog again. So, feeling very rusty, I’m going to give it a go.
My reaction to the Naviaux et al paper, Metabolic features of chronic fatigue syndrome, was dismay that the damage is so extensive and widespread. So many broken pathways. Finding a specific drug target seems very unlikely. There won’t be an answer anytime soon. They, and everyone else, including Lipkin and Hanson, are studying downstream effects, without attempting to identify the root cause. It’s a good thing that people are thinking and looking, but hibernation and dauer are not disease states and being compared to larval worms isn’t exactly the image change we need ;-). Even if they’re right and a handful of common abnormalities in this very heterogeneous group is accepted as validating real disease, my guess is that the findings will be similar in other diseases, e.g. GWI, fibromyalgia, ASD, maybe even chronic depression. GWI patients have PEM and often meet criteria for ME/CFS. As I said five years ago, I think all of these diseases of modern civilization are related and there is a family factor that confers risk to partners and offspring. There are even a few patients who believe themselves to be contagious by casual contact.
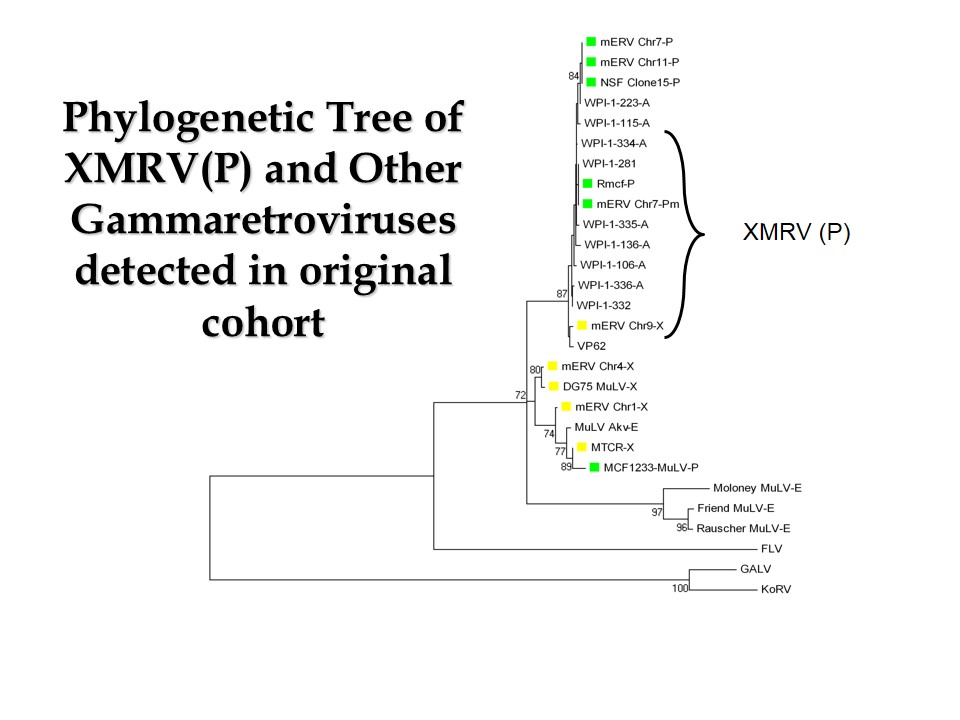
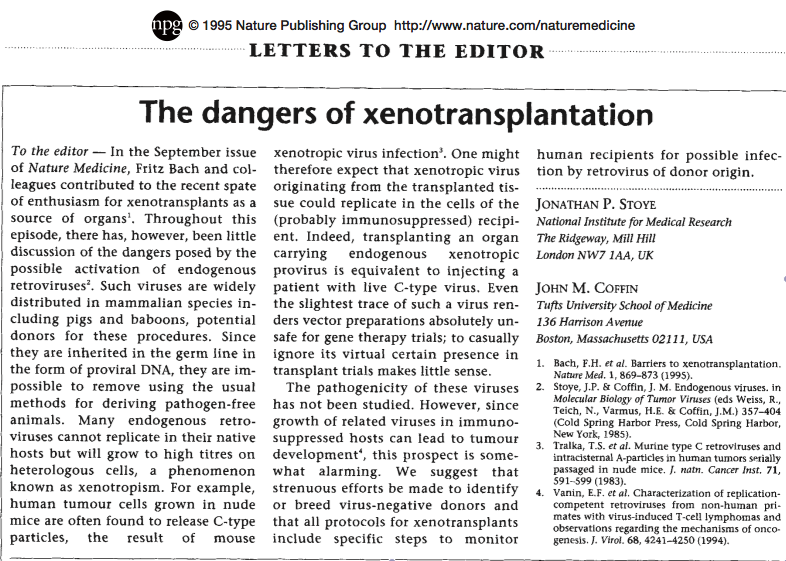
So what lies in wait to be activated by heterogeneous triggers and once activated causes immune dysfunction, neurological disease and opportunistic infections? The most likely explanation lives in the realm between retrovirology and genomics, the difference between the fields being as small as a single mutation. We have been injecting retroviruses and pieces of retroviruses into people for over a century. What are the chances that nothing bad happened from that? XMRV apparently doesn’t infect people, but injected into monkeys, it sets up a low level infection. Retroviruses recombine and rescue each other. Environmental toxins activate retroelements (HERVs and retrotransposons) which can recombine with each other or new incoming retroviral sequences and fully replicative retroviruses from vaccinations, biologics and lab workers. XMRV was created in a lab. The Paprotka paper said the odds of the recombination event that produced XMRV happening twice are infinitesimal. On the other hand, the odds of similar events having happened many times is very high I would think, since there have been so many chances. In the last few years it has been found that many cell lines produce viruses like XMRV which are capable of infecting human cells in tissue culture. Lipkin said in a press conference that 85% of Montoya’s samples contained retroviral sequences and in the XMRV study, 6% of patients and controls were positive for an antibody to SFFV, a very nasty murine retrovirus, but everybody is choosing to ignore those clues because that well is poisoned. Nobody wants to be the next Judy Mikovits. Lo and Alter both dropped it like a hot potato, returning to other research, never mind the question of how all these labs, Mikovits, Ruscetti, Silverman and Lo/Alter managed to consistently contaminate the patient samples at a higher rate than the controls.
Take a look at this paper: Are human endogenous retroviruses triggers of autoimmune diseases? Unveiling associations of three diseases and viral loci by Bjørn et al. “We speculate the possibility that recombinants or mixed viral particles are formed and that the resulting viruses stimulate the innate immune system, thereby initiating the autoimmune response.” They looked at multiple sclerosis, type 1 diabetes mellitus, and rheumatoid arthritis. It is one of several recent papers heading in this direction.
I hypothesized way back when that ME/CFS is related to MS. There are case reports of MS improving when patients take antiretrovirals, Multiple sclerosis patient walks after taking HIV drugs, and new cases of MS are rare or nonexistent in patients taking AIDS drugs, HIV and lower risk of multiple sclerosis: beginning to unravel a mystery using a record-linked database study.
Our very own Gerwyn Morris published an excellent paper on the subject of ME and MS being related diseases. Myalgic encephalomyelitis/chronic fatigue syndrome and encephalomyelitis disseminata/multiple sclerosis show remarkable levels of similarity in phenomenology and neuroimmune characteristics. I’d like to take this opportunity to acknowledge Gerwyn’s extraordinary achievement. If you search “Morris Gerwyn” on PubMed, his name appears as an author on 23 papers since 2013, usually as first author.
Lots of evidence has been published about the MS retrovirus, MSRV. Viral particles have clearly been detected, but it is less clear if these particles are ever infectious. There are several new papers reporting findings similar to this one, Two endogenous retroviral loci appear to contribute to Multiple Sclerosis.
Which brings us back to where this blog began. Are retroviruses at the bottom of ME/CFS? Might antiretrovirals be effective for ME/CFS and other diseases? Despite the thorough trashing of retroviruses in our disease and the intense ongoing fear mongering about how dangerous antiretroviral drugs are, apparently people are still trying it in Europe. The experience five years ago, when maybe a hundred people tried various regimens in a completely uncontrolled fashion, was some subjective improvement in about half, and no complete recoveries, except for one notable exception. The exception was a teenager who had only been sick for eight months. His mother wrote in the comments on this blog. He recovered fully, took the drugs for 6 months, stopped and as far as I know, didn’t relapse. I still find it upsetting that the prescribing physician was too cowardly to come forward and write a case report. How many teenagers could have been treated acutely since then? There were no injuries that I ever heard of. I was in touch with many of the doctors who were prescribing and there was lots of sharing, doctors and patients together, the only time I’ve ever seen that happen. One doctor I knew prescribed for 50 patients and concluded that it was better than placebo, but not worth the risk of prescribing it.
However encouraging the Naviaux paper may be with respect to advancing the case that ME/CFS is, in fact, a real and dreadful disease, it is discouraging with respect to finding treatment. A viable drug target seems unlikely. We are left with global strategies, hoping for synergy between therapies that don’t stand alone, same as now. But just as I was feeling dour about dauer…
The NIH compilation of responses to their request for proposals was published here. Read bottom of page 3 to top of page 4. I’m not going to mention any names for Google, because I don’t want to increase the risk of regulatory repercussions against a doctor brave enough to report successes with antiretrovirals. Also please read pages 9-12.
Then I heard from a patient in Europe who is having success with antiretrovirals after 20+ years of illness. In his own words:
I have been ill with ME since my mid-teens in 1994. Onset was in two stages. Firstly a gradual onset, whereby I was feeling increasingly more tested after the combined measleas/rubella vaccine, followed a few weeks later by the polio booster. And then secondly once that prodrome had got its hold, the downward cascade was always inevitable, and just waiting for me around the corner. 1994-2014 were harsh and brutal years. I hovered around 55% on the Bell scale and it was torture enough.
From September 2014 to July 2015 I took tenofovir 245mg. Improvement was an upward curve, albeit with some turbulence. Sometimes taking half- week, or full-week, or month-long breaks when I felt my body needed a rest from it so as to hold its own for a while. From August 2015 to September 2016 I added raltegravir to tenofovir and initially at full dose daily which sent me to sleep almost in the first few days. During this period I toggled around until I found the right balance for me. I got it right in the end around about June/July 2016 and the past two/three months have been great. My current regimen is tenofovir 245mg Tuesday through Friday, and on Tuesday and Thursday I also take raltegravir 400mg x 2. My original baseline was about 55% on the Bell scale for the twenty or so years when I was sick. I am now 95-100% and can go to the gym once weekly thanks to the antiretrovirals where I can build up quite a healthy sweat and recuperate normally. My VO2 max continues to increase substantially and my CD3-4-8 counts are x2.5 to 3 fold what they were before I started the antiretrovirals. Life is very good. I also take celebrex and multivitamin/antioxidant supplements and I am monitored closely.
This year I feel more confident about the winter than I did in 2014 on just tenofovir and than in 2015 when I was grappling with adding raltegravir. They were bad winters even though the arv’s did help me through better I guess. Winter 2016 can throw at me what it wants however. Now that I have hit the perfect treatment regimen with the antiretrovirals I am sure it will be a better winter. It was worth sticking it out and learning. I thank Dr Judy Mikovits and my physician over in Germany, along with the continued support of a rare and dedicated French doctor over there in Paris. Finally I thank two doctors over there in the UK for listening. I salute them all as men and women of true honour.
Several people wrote to ask what happened with antiretrovirals for my daughter and me. Ali and I plateaued without recovering fully. After the initial improvement, there was really no way to know what was happening. We both had a very mild flare of symptoms for the first six weeks and then a noticeable increase in energy and resilience. We started with AZT and Isentress, then switched the AZT to Viread a year later. Ali stayed on the two drugs for three years, not wanting to rock the boat, as she was doing relatively well. I stopped the Isentress after about a year and half and took Viread alone after that. We both improved during the three years we took antiretrovirals, but we were doing lots of other things documented on this blog. Since there was always the possibility that we might do better without them, eventually we decided we should find out. As it turned out, we didn’t decline when we stopped. I had some trouble coming off Viread, because my always labile blood pressure went crazy when I stopped, twice. Go figure. In the end, I weaned without any sort of noticeable decline. When we started, we were all so hopeful. Judy believed we’d be able to monitor viral load in a year, but it wasn’t to be. Our combined copays were breaking the bank and after three years, with no way to monitor and able to stop, it just didn’t make sense to continue. I would consider antiretroviral drugs again if either of us crashed completely.
My experience treating six very informed patients was similar to what other doctors have reported, 50% improved subjectively. Two had adverse reactions to Viread, including one who had responded initially; both resolved quickly when the drugs were stopped. Two patients continued long term, one on two drugs and one who opted for Viread monotherapy. I didn’t see anything dramatic enough to make me very encouraged though. I had successes with other things that were similar in scale with less risk to the patient and the doctor. However, it’s possible that tinkering with lower doses and less than every day regimens would make the drugs we have more useful for ME/CFS, even if they were designed for a virus we don’t have. Although we do not want to encourage resistance to the drugs, it’s possible that a small dose of a reverse transcriptase inhibitor would work for us. I heard from a doctor in Europe who reported complete recovery in 2011 after nine months on micro dose AZT (20-30mg/day). I don’t know how it turned out long term, but will write to him and ask.
Dr. Michael Snyderman is still doing remarkably well, still able to work in his hematology oncology practice at 75, controlling his cancer like a chronic disease, specifically like AIDS. He has been taking HAART for over 6 years, having twice passed his median survival, meaning there was less than a 25% chance that he’d still be alive by now. I will share his data here in the near future. He is still hoping to collaborate with Roswell Park Cancer Center in his hometown of Buffalo, NY to help patients who have cancer and who have a poor prognosis. The same viruses that infect cancers infect the immune system. If cancer patients benefit as he expects they will, initiatives can be made with the neuroinflammatory disorders including ME/CFS. There is now a reliable virus detection methodology, ViroCap invented by the Wylies at Washington University and the Wylies are interested in collaborating with this research.
These are leads, the only leads we have. If drugs developed for a completely different retrovirus have some activity against a disease, think what could happen with some attention to the process that is actually occurring. The technology, next generation sequencing, already exists to begin to answer our questions, but the various software platforms that analyze the data are still in their infancy. The metabolomics studies are happening because there is a new toy. There are going to be lots of new toys in the near future. It already didn’t happen by random doctors prescribing off label. Since it wasn’t a slam dunk, it needs to be formally and properly studied.
It is possible that the metabolites that Naviaux et al have identified as a potential diagnostic panel might be useful for monitoring success with antiretrovirals. Dr. Naviaux has answered questions here, stating that he thinks the use of antibiotics and antivirals aren’t indicated and I mostly agree with him, planning to share my thoughts on treatment in a future blog.
I continued to go slowly uphill after I last blogged about ME/CFS almost two years ago, but nothing like a full recovery. I was able to work a little and I was able to ride on the back of a tandem, close to a thousand miles in two years according to Strava, half of it on dirt. Still lots of symptoms, but a life, where once there wasn’t one, plus a way to get endorphins. My recovery was slow after exercise; I felt drained the next day, but nothing like full blown PEM. I was still maintaining the fantasy that someday I would recover fully. But a year ago, while hiking, I twisted my ankle and broke my distal fibula. It was a minor fracture that should have healed without problems in 6 weeks. Instead I got RSD/CRPS (reflex sympathetic dystrophy/complex regional pain syndrome), a very challenging and painful condition. It takes most of my energy just to cope and I’ve been out of commission since it started, able to attend only to my own treatment (HBOT).
After 5 years of managing patients, I had to retire completely. I only worked with a very small number of patients, scattered all over the country, who saw me in person once a year in Hawaii or Arizona, but I got to know them very well, because most of the contact was electronic, day to day, moment to moment even, and that works well for ME/CFS patients. It was enough to learn quite a bit about the spectrum of disease, what works and what doesn’t, especially given that almost everyone I saw had been around the block and came with voluminous records, having failed treatment with the best. I’d like to share my impressions while still fresh, so intend to keep blogging, if I don’t get too beat up over this one ;-).
Today’s song from Les Misérables