Last October, after three months on the Wahls paleo diet, I recovered my ability to benefit from exercise. I had been unable to exercise without payback for nine years, since starting treatment for tick borne diseases, a decade into my illness. That most intangible switch between can’t and can suddenly flipped back and aerobic exercise became possible again. No drugs involved. Just a clean, nutrient dense, low carbohydrate diet. Lots of healthy fat.
In February, the “flu” went through our house. I was down with it for about 6 weeks. Then I pushed through and went to Tucson to see patients in April. My upper respiratory tract symptoms came back on my second day home and a week later my husband got sick also. Then, in quick succession, I had a UTI, sinusitis and a salivary gland infection requiring back to back courses of antibiotics.
My mood crashed also. It’s really tough to be very active for a while and then find yourself back in the pit. When I was emerging from years of hell, I felt amazingly wonderful, even though I still had lots of symptoms. Conversely, after a period of very few symptoms, I had a lot of trouble coping with symptoms that would have been no big deal when I was sicker.
I don’t usually catch stuff. I’d been experimenting with higher doses of Vitamin D after reading some studies about using higher doses in MS patients for anti-inflammatory effect. In hindsight, the dose I was taking was probably too immunosuppressive for me, though it is cited as safe in several recent papers. When I went back to a lower dose, the infections stopped. I didn’t try this experiment on anyone but myself. If you do try higher doses of Vitamin D, follow levels and be careful. Upward target level creep is happening in the literature, as people try to use Vitamin D as a drug, not just a preventative. For me, 5000 iu daily seems OK and my 25(OH)D level on that dose is about 50 ng/mL. More was not better, but I am not saying that it couldn’t be for someone else. The word isn’t in yet as to how to supplement Vitamin D optimally in the setting of neuroimmune illnesses. Natural sunlight is no doubt the best way. The most powerful ways to heal are provided by Mother Nature, not a pharmaceutical or neutraceutical company.
Despite my fear that the gig was up for good this time, gut torn up again by antibiotics, I started the climb back to wellerness. I was really weak when I got back on the bike, but I improved faster than the first time and by early August had surpassed my previous level. Anthony and I spent our 26th anniversary camping on the Conejos River in southern Colorado, and went fishing in our canoe on Platoro Reservoir, same as our 25th. Last year, I needed a special seat on the floor of the canoe with a backrest. This year, I could help paddle. Last year, I couldn’t ride a bike. This year, we rode uphill on a fire road for an hour, from 9000 to almost 11,000 feet, before a long, exciting descent. Then later, the same day, we went fishing. If you have been reading my blog for a while, you will recall, I used to need a wheelchair to get through an airport. Now I could jog to the gate if I were late. Exercise is my go to “treatment” when I am feeling poorly, which I still do, not infrequently. I am not cured, by a long shot, but I’m not at the mercy of the illness. I can fight back.
I still attribute my recovered exercise ability to the Wahls paleo diet. I’m no longer completely adherent though. My intake of vegetables is much increased from prior, but I’m no longer force feeding. I eat some rice and quinoa and a few legumes. I eat bananas, apples and pears, though Wahls excludes them. I’ve learned that any dairy is problematic, except butter, but I can get away with a bite of gluten, at least as far as I can tell. Properly produced eggs are my friend, though I haven’t tested for egg allergy or tried eliminating them. My focus has become not only what I eat, but what I avoid, especially toxins and GMOs. We are paying attention to what cookware we use and what we store food in. Bone broth is a staple in our household. My daughter makes it with fresh turmeric root and seaweed. I love my green drinks. We are having an adventure with fermenting. We are learning what edibles grow naturally around us. I am going hunting for prickly pears with my daughter and grandchildren in a little while, planning to make prickly pear, crabapple butter. It will probably be terrible:-), but the walk and the project will do us good.
We are no longer eating as much meat as we were when we first went on the diet. We are a large family and bought a whole cow from a local ranch. It was definitely different to buy it alive and sign off on its slaughter. For about six months, we ate a large amount of very high quality, grass fed, grass finished beef. After that, two healthy members of the family had serious GI complications, specifics of which I won’t share to protect their privacy. Anecdotal of course, but we decided to back off on the red meat. We are eating more fish, even though finding clean fish is so problematic, and having more vegetarian meals.
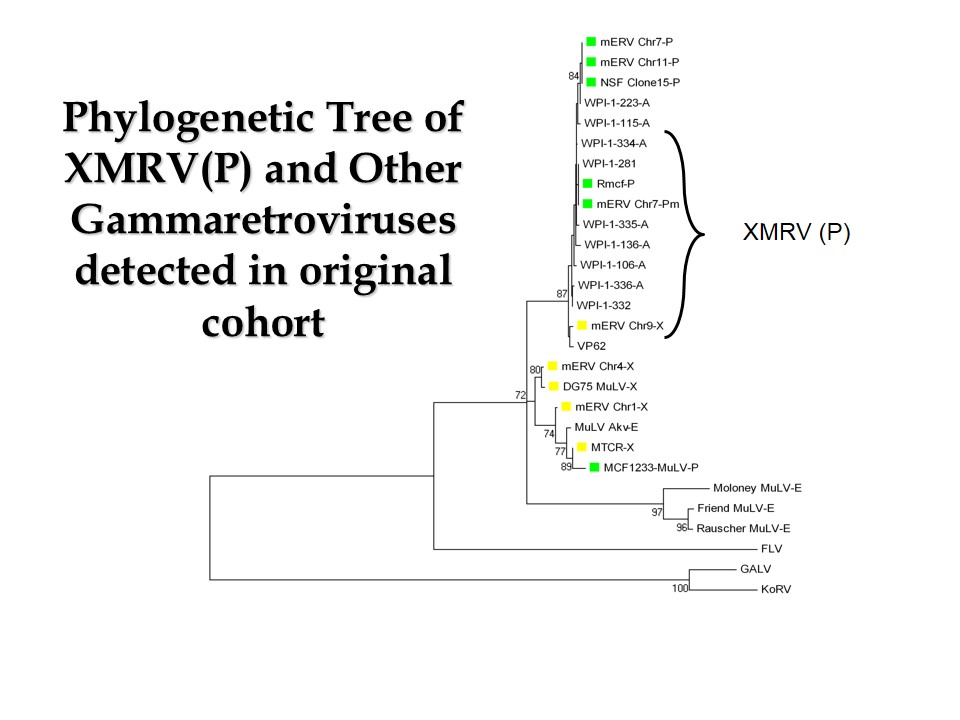
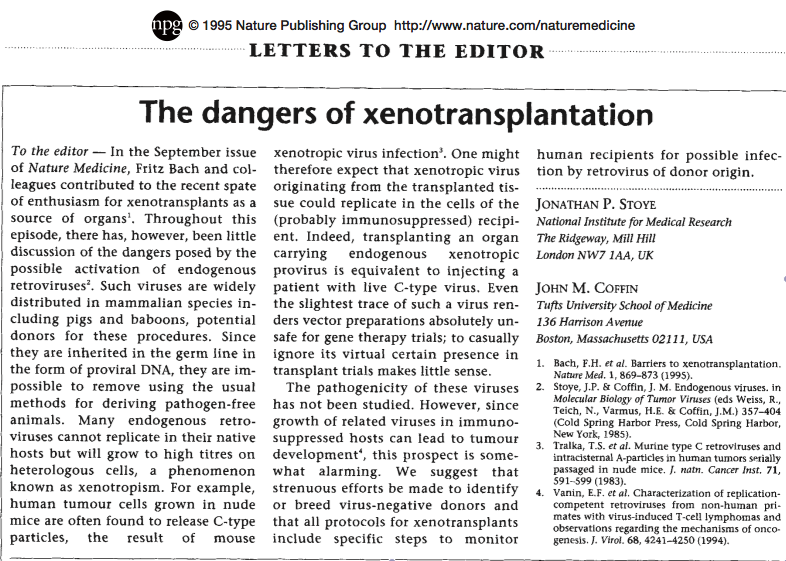
I stopped writing, not because I was too sick, but because I was too negative. Existential crisis. Jaded and cynical. Disgusted with how broken and corrupt the system is and how hopeless it seems that our current suicidal trajectory can be changed in time. We are about to be a failed experiment, on a global scale. Why write about it? Time to eat, drink and be merry. We have the technology to figure out what we need to do, and not do for neuroimmune illnesses, but no cavalry is coming over the hill. The game is rigged. All greed and special interests. What gets studied, and then published, is tightly controlled. Obvious studies that challenge a prevailing paradigm will not get done (vaccinated vs unvaccinated children or the family study we tried to do once on this blog). Scientists who dare to depart from the mainstream paradigm are discredited (Mikovits and Ruscetti). Yet real live fraud within a government agency that most likely harmed children is covered up by the media (see my last blog). The billions of dollars paid out by the drug companies for their frequent gigantic frauds make the news, but their stock prices remain strong. Those billions are just the price of doing business. And they are indemnified in the case of vaccines, so that’s a real gravy train. The medical profession is completely asleep at the wheel when it comes to the causes of or solutions to complex chronic diseases. Safe treatments that can’t be patented, like home oxygen, will never be studied. So their treatments now do more harm than good. Conventional doctors push dangerous drugs. Alternative doctors push expensive tests and supplements. Depressed yet? I certainly am, if I think about it too much. So I won’t. I’ll go on a hike with family at the end of a magnificent monsoon season in the high desert, pick prickly pears and be grateful I can walk. Time to find some heavy gloves.
Stay tuned for an update from Dr. Michael Snyderman.
By Way of Sorrow – Cry, Cry, Cry