
Even though the last blog was the least controversial I’ve ever written, it managed to ruffle a few feathers. On the one hand, it couldn’t possibly be as simple as a diet cure and, on the other, it is too hard to implement, especially if you are sick and short of money. And what about retroviruses?
I am not cured. It is a relapsing, remitting illness and I am experiencing a remission. I am not asymptomatic, but much, much better. My husband and I have ridden our tandem 180 miles so far this month. Our rides are quickly getting longer, faster and more challenging. My husband said I have never worked harder. I don’t know if that’s because I want it more, or because I finally fixed my rubidium deficiency;-). No doubt a real doctor would say I finally decided to get off my ass;-). But anyone with real knowledge of the disease knows what a profound change has to occur for an ME patient to return to exercise after nine years.
Ali also has noticed improvement with respect to her physical abilities. She went to an hour long yoga class a few days ago with no PEM and expects to continue. She is living away from me, something neither of us thought possible just a few short years ago.
It isn’t just the diet. The diet happened to us in the context of a slow recovery over a number of years during which several treatments were contributory, all documented on this blog. Antiretrovirals, oxygen, Deplin, at one time Actos, at another modified Meyer’s cocktail IVs, metformin and Prometrium for Ali, prior dietary modifications and ever more awareness of the importance of biotoxin avoidance. I believe all of these things have helped to tip the balance towards recovery. When you are treating an incurable disease, it is necessary to look for therapeutic synergy.
As to the diet being hard, some of the biggest things aren’t too hard. A daily smoothie, big plates of organic greens, bone broth from clean grass fed animals. Buy organic. Try your local CSA (community sponsored agriculture) who sometimes deliver. Try eliminating gluten and dairy for three months. Consider nutrient density before eating something. Don’t try to change everything at once. Pick one thing and do that, then add to it. It is more expensive to eat this way. If it is too expensive, I am thinking the food is more important than supplements, on which most patients spend a lot of money. I am increasingly suspicious of things that come in pill form, including supplements.
One of the really interesting things that has happened to me on the Wahls diet is I am not tolerating B vitamins at all, finding them overactivating and sleep disrupting, after taking Deplin for years. I presume this is because I am getting what I need from my food. Can we infer from this that my methylation status has improved? Take a look at the numbers midway through this article by Dr. Wahls: Maximizing Nutrient Density for the Modern Day Hunter-Gatherer.
In addition to a relatively small number of known required nutrients, whole food contains thousands of compounds which work together in ways we do not begin to understand. Supplements supply an excess of a single nutrient. In the case of L-methylfolate, the idea is to overcome an enzyme deficiency by supplying the activated form of the nutrient folic acid to prime the pump of essential metabolic pathways. The deficiency occurs more often in the presence of certain genetic mutations, or SNPs, but remember, the problem is most often not caused by the genetic make-up of the individual, who was healthy once, but by epigenetic changes that have occurred. Also remember that methylation silences retroviruses.
I still think retroviruses are at the bottom of it, endogenous and/or exogenous. I will prevail upon Dr. Snyderman, who has lots to say on this subject, to give us an update in the near future. There is a growing body of literature to support the association of activated HERVs with various diseases. There are even a few intrepid researchers still pursuing novel retroviruses in chronic disease, working at the edge of our current understanding. Andrew Mason‘s betaretrovirus associated with primary billiary cirrhosis, clinical trials with antiretrovirals ongoing, Sidney Grossberg‘s JHK gammaretrovirus which he has identified in CFS patients, and Hervé Perron‘s MSRV, particles from HERV-W transcripts, with an immunopathogenic envelope protein, severity of illness correlates to viral load, replication competence still unknown. “Most HERVs are unable to replicate but MSRV expression associated with reverse-transcriptase activity in MS would explain reported DNA copy number increase in MS patients.” from The DNA copy number of human endogenous retrovirus-W (MSRV-type) is increased in multiple sclerosis patients and is influenced by gender and disease severity.
The possibility that animal retroviruses are the root cause of the enormous increase in chronic neuroinflammatory illnesses, autoimmunity and cancer in our modern world has not been ruled out, just because the particular sequence called XMRV has been put to bed. In fact, in figuring out where XMRV came from, created in a lab using techniques in use every day all over the world, a can of worms has been opened. How many times have similar organisms been created? How many cell lines commonly in use produce infectious virus that can spread airborne through a clean lab, as XMRV does.
Given that retroviruses recombine and rescue each other, that under certain conditions HERVs activate to produce viral product, that the environment is full of the very toxins used to amplify retroviruses in the lab and that high risk biotechnologies have offered up so many chances for new retroviruses to infect humans, it seems more likely than unlikely that it has happened, and more than once. After all, we have been injecting adventitious retroviruses into people for 80 plus years in combination with other live viruses. We think nothing of fusing human and mouse genetic material to produce monoclonal antibodies that are given to immunocompromised people. Passaging human tumor tissue through immunodeficient mice, gene vector technology, genetically modifying animals to produce human proteins for IV administration (Atryn) are all very high risk things to do. Lots and lots of chances. Hubris allowed it. Money drives it. How could the legacy of all that science be that half of everybody has a chronic illness, including children? Who wants to know that?
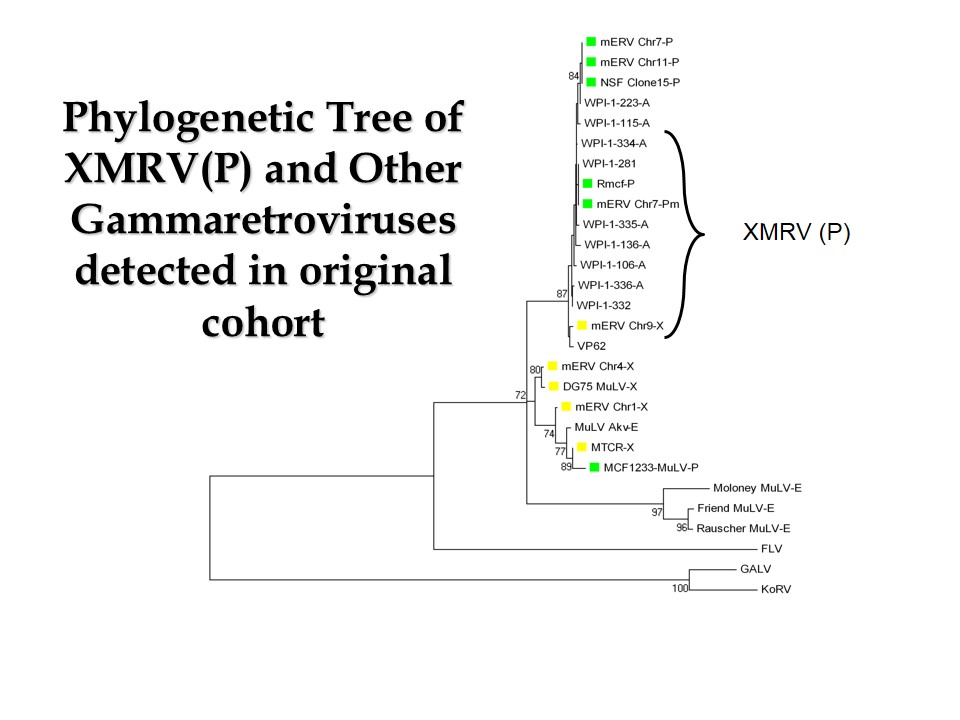
Injected into monkeys, XMRV causes a low level latent infection, which isn’t communicated by transfusion. However, Dr. Mikovits found other sequences in patients besides XMRV. Here is a slide from her recent lecture at Dr. Enlander’s conference showing just that.
Of course, she doesn’t have her notes, so all of the unpublished work she did is lost to us. Meanwhile, the WPI continues to suck up a big chunk of the government dollars spent on our disease, while their co-founder awaits jail for his felony convictions.
$450,000 of taxpayer money was spent on the specimens collected for the Lipkin study, which was negative, as expected. The good news was that Dr. Lipkin was going to use those specimens to answer some questions. I guess he couldn’t get funding. Instead those specimens have gone to Dr. Peterson, who is raising money to look for evidence of arthropod borne disease, even though the collection criteria for the specimens specifically excluded Lyme Disease. How’s that for looking under the streetlight?
Meanwhile, as a patient community, we are back to case definitions, an obfuscation if there ever was one. A case definition is an exercise in futility, because the disease isn’t one thing. ME/CFS is a garbage pail diagnosis, somewhere to put all those patients who feel awful, have non-specific immune dysfunction and secondary mitochondrial failure, with nothing else to define their illnesses. Many roads lead to Rome. The question of causation is simply too complex for our current scientific methods. The ability to analyze huge amounts of genetic material cost effectively is coming, but it isn’t here yet. It may turn out that the specific retroviral sequences involved are found in particular families or groups of people with certain environmental exposures, e.g. certain chemicals or vaccines.
With the burying of XMRV has come a resurgence of Lyme Disease as The Cause. The CDC recently admitted that they were low on the number of annual cases by a factor of ten, right on time for the release of Baxter’s new vaccine and Lyme test. The CDC’s admission is unfortunately a boon to ILADS, a renegade medical society based on an incestuous relationship with a private lab, to which they refer and then use the unvalidated results to perpetuate their mythology: Patients congratulated for “herx” reactions to antibiotics, rather than recognizing it for the damaging cytokine storm that it is. Then there’s the one about how enough antibiotics in the right combination for the right duration can eradicate it, despite all evidence to the contrary. And the one about how chronic Lyme Disease is a distinct entity from ME/CFS, despite the fact that the two groups are clinically indistinguishable without test results from this one particular cash only lab whose results no other lab can duplicate. And then, if they happen to get a negative test, which is a rare event, the most imaginative of all, seronegative Lyme can be diagnosed clinically, even in people with no risk factors. It’s a scam and a dangerous one. I saw this yesterday: Is Lyme Disease Contagious? Clues Hint That It May Be A Sexually Transmitted Disease, quoting no other than Dr. Raphael Stricker, the most published of the so called LLMDs. Here is what the Office of Research Integrity at the NIH has to say about him (link):
Raphael B. Stricker, M.D., University of California at San Francisco. An investigation conducted by the University found that Dr. Stricker falsified data for a manuscript and a PHS-supported publication reporting research on AIDS. In the manuscript, Dr. Stricker selectively suppressed data that did not support his hypothesis, and reported consistently positive data whereas only one of four experiments had produced positive results. In the publication, Dr. Stricker reported that an antibody was found in 29 of 30 homosexuals, but not found in non-homosexuals. However, Dr. Stricker”s control data, which he suppressed, showed the antibody in 33 of 65 non- homosexuals. The falsified data was used as the basis for a grant application to the National Institutes of Health. The ORI concurred in the University”s finding. Dr. Stricker executed a Voluntary Exclusion and Settlement Agreement in which he has agreed not to apply for Federal grant or contract funds and will not serve on PHS advisory committees, boards or peer review groups for a three year period beginning April 1, 1993. The publication “Target platelet antigen in homosexual men with immune thrombocytopenia” in the New England Journal of Medicine, 313: 1315-1380, 1985 has been retracted (New England Journal of Medicine, 325: 1487,1991).
ME/CFS, Chronic Lyme Disease, mold illness, MCS, fibromyalgia, GWI, all have pretty much the same symptoms. Lots of tunnel vision going on in each group. A retroviral hypothesis is the most parsimonious explanation for all of these diseases, which didn’t exist or were very rare when I went to medical school 35 years ago. Dysautonomia, now common, wasn’t seen then except rarely in advanced diabetes. A retroviral hypothesis fits for ASD also. This very brief distillation is all referenced elsewhere on this blog. However, even when one turns to the literature for answers, you have to figure that a very large proportion of it is wrong due to mistakes, contamination and fraud (lots of that going around). Why Scientific Studies Are So Often Wrong: The Streetlight Effect. So whatever cohort you fall into, which may depend more upon which doctor you go to than anything else, you get to choose between neglect by conventional doctors and expensive overtreatment by the “experts”. My advice is avoid doctors and eat your vegetables.
Tonight’s song: We Shall Overcome by Pete Seeger
Thanks for another interesting blog Jamie. I am so glad you have made further improvements and Ali too.
Regarding antibiotics causing a cytokine storm, I am still not clear how this works. Why do antibiotics cause a cytokine storm? Is it because in their very nature antibiotics kill off whatever bacterias are around and this causes the immune system to ramp up? Many thanks.
I have finally managed to completely come off zopliclone. I still take 10mg amitriptyline for sleep but at least I am off one sleep med :-)
Your question about Jarisch Herxheimer reactions is a good one, Annie, and I’ll write my thoughts about it in a near future blog. I started to write more about Lyme in this one, but it was getting too long and it is a painful topic for me, since I really went down the rabbit hole myself.
Congratulations on getting rid of a drug. They are almost always a double edged sword, especially with respect to sleep.
Thanks Jamie. I would really appreciate a blog explaining more about how the alleged herx reactions in long term abx may well be a cytokine storm and why abx can cause this cytokine storm.
I am sorry knowing you have been down the rabbit hole of years of antibiotics with bad consequences it may not not be an easy topic for you to revisit but it would be very helpful and appreciated.
I appreciate you making it clear that you put your improvements down to a synergetic effect with the various things you have tried and continue doing allowing your body to shift into a positive direction and may it continue. I suppose my one question is although I know you would say antiretrovirals meds alone would not have got you where you are, is it possible diet alone would not have allowed you and thus others to not progress as you thankfully have? I also appreciate the current antiretrovirals on the market may not be ideal for whatever it is we have.
Is it a case of perhaps the best case scenario would be to have access to antiretrovirals as well as doing the diet, oxygen and so on but as most of us cannot access antiretroviral meds then as we can try the other approaches, including diet, it is worth trying as it may be enough to shift our illness in the right direction towards remission? Many thanks
Don’t think Lyme, think Borrelia. Borrelia is everywhere. And toss away ILADS and IDSA as considerations. If you do that, you know that no diagnostics today are without grave flaws. So Borrelia, and the impressive array of allied TBD’s, could apply in theory to many, many of those carrying anyone of the disorders you noted.
Factor in a retrovirus, and maybe that’s the toxic cocktail so many of us have unwittingly imbibed.
Isn’t that semantics? Lyme being the name for a borrelia infection?
Semantics? No. Lyme is Borrelia Burgdorferi. It is one species of Borrelia (Borrelia being the genus). There are about 35 Borrelia species. Not even sure about the number of strains. Lots. Included in that would be what is perceived as traditional tick-borne diseases like Lyme, but also Borrelia spread by lice that include a type of relapsing fever. Lots of variables. Lots of diseases. Somehow, the Lyme name became an umbrella label.
At issue are the testing mechanisms for Borrelia, which many believe are subpar. Because they are subpar, in terms of combined sensitivity and specificity, many individuals who get tested for Borrelia, e.g. Lyme, are given false negatives. If they are even tested. Many patients are not advised by clinicians to be tested because govt agencies tell those physicians the disease is not a factor in the area in which the patient resides.
There is an additional very real war being waged on the treatment front pitting IDSA vs ILADS in terms of therapy protocol.
Unfortunately, the collateral damage in that war, imo, is the many patients walking around undiagnosed.
Aach. It certainly gets convoluted quickly. But no, it cannot be boiled down to merely semantics.
I am using “chronic Lyme Disease” broadly to describe the late consequences of tick borne infections that include Borrelia burdorferi and other co-infections.
Thank you. I wasn’t aware borrelia is the genus until you explained. So obviously i was wrong to say isn’t it just semantics, apologies
To add, Duncan, I’m aware that standard testing can throw up false negatives but do you think some of those private labs can give false positives as well? Or is that an impossible question to answer? Many thanks
Annie, false positives can happen, and this is not debated. What IS debated is the rate of incidence of such false readings. Many believe the rate of false positives is far lower than that of false negatives.
Also, there is controversy over how long a person who earlier had been infected will show positive titers in his/her labs. In theory, Bb levels should decline, but I think that may hold true more (or may be more easily demonstrated) for acute cases than disseminated. Certain tests like the c6 peptide I think may support that contention, but, yes, there is debate over that, too. Not to mention what qualifies blood work as positive – many dispute CDC/IDSA governance.
Annie, Duncan replied to you but his reply is still evidently being evaluated. Why I don’t know. He’s one of the smartest people I know when it come to TBDs. I didn’t want you to think he was being rude and ignoring you. :)
Sorry, for the delay. I’m having trouble getting notifications from WordPress. I don’t censor comments unless they are spam or abusive (which hasn’t happened in a long time thankfully).
I knew that Jamie. And I’m very thankful for that as I’m sure other are as well. I didn’t want Annie to think Duncan was ignoring her while at the same time I thought it would notify you to any potential problems with your blog. Thanks again for all you do!
Thank you, very kind of you. All understood now :-)
And let’s not forget that one thing both Borrelia and ME/CFS have in common (besides an eerily similar symptom cluster) is a comically grim mishandling of both – some might say deliberately so – by governments around the world.
I am not ready to toss chronic borreliosis out the window. IF it functions in a similar way to it’s cousin, syphilis, then tertiary borreliosis would be untreatable. I got a bull’s eye rash following a tick bite 20 years ago and never got a single antibiotic for at least 2 years after the bite.
As to that unmentionable lab, I had several positive bands on the western blot years after that tick bite and many antibiotics. Then I had a positive urine antigen test for borrelia after a week of Zithromax.
Am I still in the band for a retrovirus or three? Yes. Have I quit the ILADS band for chronic Lyme disease? No.
It isn’t the diagnosis that needs to be tossed. It is the organization that is the problem. There is no intellectual honesty about their results. They exist as a reaction to IDSA and that has colored their thinking from the beginning. When I quit ILADS 5 years ago I was reassured by their then president that they were revising their guidelines from 2004, but it hasn’t happened. They continue to push an open ended protocol that can be extremely dangerous. It does seem that a few of their own celebrity status doctors are finally saying it doesn’t work so well, beginning to realize that they are dealing with an underlying immune dysfunction. I hate writing about Lyme Disease, because I am always misinterpreted to be saying that Bb and other TBDs aren’t a problem, which couldn’t be further from the truth. It is the approach to treatment and not taking responsibility for bad outcomes that I am taking exception to.
Unfortunately, I agree it does seem if you acknowledge Borrelia as an ongoing issue, you have to state an allegiance to either the IDSA or ILADS. As you well know, and have spoken to so finely in the past, swearing off one does not necessarily mean you don’t want to jettison the other as well. :)
I have major problems with both, so I try to focus on the Science. I have sworn off either camp’s interpretation of any thing TBD till I run it though my own grossly inadequate acid tests. I think the Science is there from back in the 80’s and early 90’s. It’s the interpretations and the mercenary politics that govern them that haunt progress. No surprise there, though, I suppose.
Regardless of loyalties, and because of the appalling history of diagnostics, there is very likely many, many sick people out there with some sort of Borrelial infection. How many unknowing individuals with late stage Lyme, or some other tbd like babesiosis? How many walking around in a given State or Country without any clue simply because a resident govt agency isn’t advising clinicians to look for it, or worse, advising them it cannot exist there?
I prefer not to speak to therapies (mostly because I don’t think very highly of most). Right now I am concerned about identifying everyone who actually has a tbd, and I fear there are a lot. The CDC announcing a tenfold increase in the US is a step in the right direction – but then again I smell a vaccine in the air, so there may be that consideration. Compound that very basic concern about the prevalence of Borrelia with how Borrelia may or may not interact with a ERV, and it gets dicey very quickly. But I have to wonder if there is interplay there, and I know I’m not alone in that speculation.
I hear you, really I do. Years of mega antibiotics are not the cure. But we are in a complex mess – what else is new.
What about cases like mine were the patient went years untreated?
If the lab is so poor how do we get positive western blot bands or antigen in the urine? Are they faking these lab results?
We have no good lab tests for co-infections. None.
What is the ketogenic diet doing? Why does it help some patients? Is it because they are gluten intolerant? Does the ketosis state help the brain?
Then I have to ask myself why I never saw the handwriting on the wall, when my son fully recovered on 4-5 months of oral Cefdinir, Chinese herbs and Garlicell? We are in a complicated MESS!
Happy St. Valentine’s Day! Today I washed my old car and polished it. First time in one day since ’97, by cracky! I still have no clue about CFS/ME/whatever. It is nice to have some of my life back. Hope you all find your way out of the jungle. No gummints are helping… they are just part of the jungle ;)
I have no clue how I got out. Same about how I got in. My life makes a sorry science fiction story.
It is sunny and warm in Dallas. Take heart! You may survive this little plague. A few do.
I am now on a low cholesterol diet. The doctors never give up. I did, once upon a time… this time I am trying to cooperate.
Al
The true autoimmune nature of this disease will be elucidated by DeMeirleir and Lombardi. They are years ahead. They are very aware of presence of HERV proteins and are looking into why these are expressed. I wish I could understand why everyone else has suddenly jumped on the Lyme bandwagon
Jamie…I would like to know your thoughts on Lipkin’s upcoming microbiome study.
Hi Jamie. So glad you and your daughter are doing so well. A question: since you are feeling much better, I am wondering if your blood work has also improved; I am sure the inflammatory markers are down, but has the NK cell function improved? My understanding is that normal levels are 60 – 80 Lytic Units. I imagine this has not improved too much, since the underlying autoimmune process is likely still ongoing…?
Thank you:)