Hoping that everyone can relax a little, here’s yesterday’s song that I couldn’t figure out how to post from my iPhone. We could use a little levity, I think.
When I started writing this blog, it was with a sense of astonishment that the physicians treating the patients, Lyme and CFS, didn’t seem to recognize that they had a new quiver for their arrows. The few that did were quickly censured, or swore a few patients to secrecy. I had been housebound, sometimes bedbound, for years and never expected to return to work, so I didn’t care who I pissed off. Anything was better than the isolation. The good thing about not caring was that I learned to write authentically.
During my 25 years in practice, I didn’t interface at all with the scientific community. Doctors only. I had no idea about the realities of this parallel universe that so impacts what clinical choices are open to us. I thought that the Science paper would be hailed as a great breakthough; scientists and doctors would come together, bringing different things to the table. The pace of progress would accelerate. If only that had happened!
The scientists that I’ve criticized by name were Coffin, Stoye and Racaniello. The first two put themselves out there very early on in a way that appeared designed to stop progress. They also have a long history of publishing things together that minimized the risk, so aren’t clean on the issue and their opinions shouldn’t carry much weight. Dr. Coffin also took it upon himself to try to limit treatment options, my pet peeve.
Professor Racaniello is a media figure, so fair game. I admit to being influenced by hurt feelings in his case, because I wrote to him when I started arv’s, in the midst of the first blush of excitement, wanting to have a discussion with him about the science and he shut me down, much the way Jason did. And to me, the tee-shirt still seems over the top thoughtless, though I think now that he probably didn’t understand what he was doing. There are signs that he is growing, e.g. publishing Dave Tuller’s important piece on his blog.
I was angry at Dr. Singh when she published her negative paper, for the reasons I expressed back then, but essentially the same thing again; scientists trying to call the clinical shots, though in this case I understand that she felt that her former paper was too strongly in favor. I sent her testimonials from patients improving on arv’s at that time. My understanding from Dr. Enlander is that she is back on the case. I thought her a lovely person when I met her and I am glad she is again working on our behalf. The Mt. Sinai initiative is very exciting. It is difficult not to fantasize about Dr.’s Shadt and Lipkin putting their heads together.
And Jason. Sorry Jason, I didn’t mean to hurt your feelings. I hope you learned something from our scuffle. No hard feelings on my end.
I hope I haven’t forgotten anyone. A virtual olive branch offered to all, even those most aghast at my choices…
Believe it or not, there are scientists that share with me, and I protect their privacy. I swear I’ll disavow knowledge of our friendship to my dying day if that’s what any scientist willing to share wants. At risk of scaring off the people we want to be here, there is a tracker on the blog, that allows me to see the IP address, location and the name of the server that loads each blog page, as well as how many prior visits from that address. Institutional servers give the name of the institution. There are at least a dozen readers at the NCI and another dozen who connect from NIH servers in a few different cities. A couple at the CDC in Atlanta. Readers at many universities and teaching hospitals, including a few at Columbia and Harvard. Cancer institutes around the country. Only a few of these people participate in the discussion. This is a potentially powerful thing. When I worked for the WPI, one of things I most wanted to do was establish lines of communication between physicians and scientists with all kinds of points of view. There is little to be learned from consensus when the truth isn’t even on the table. If there is a way to salvage some part of that dream, I’d like to.
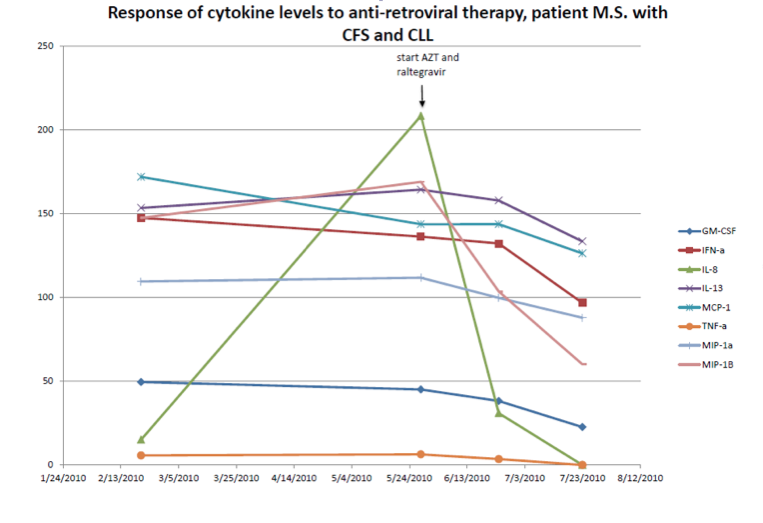
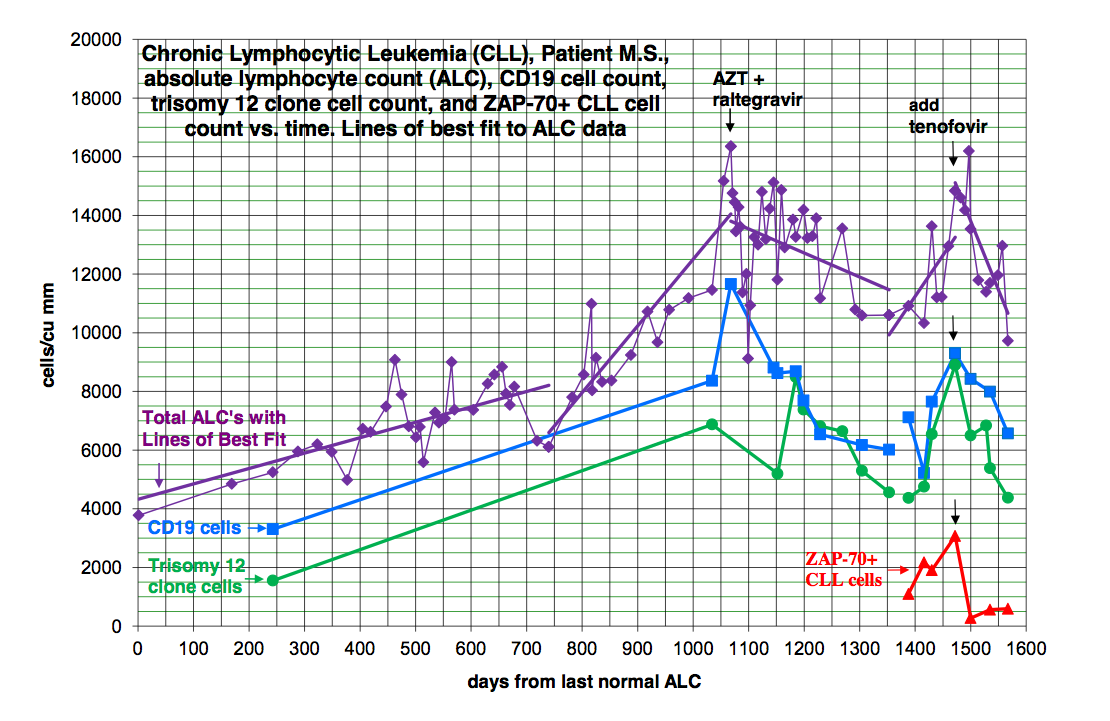
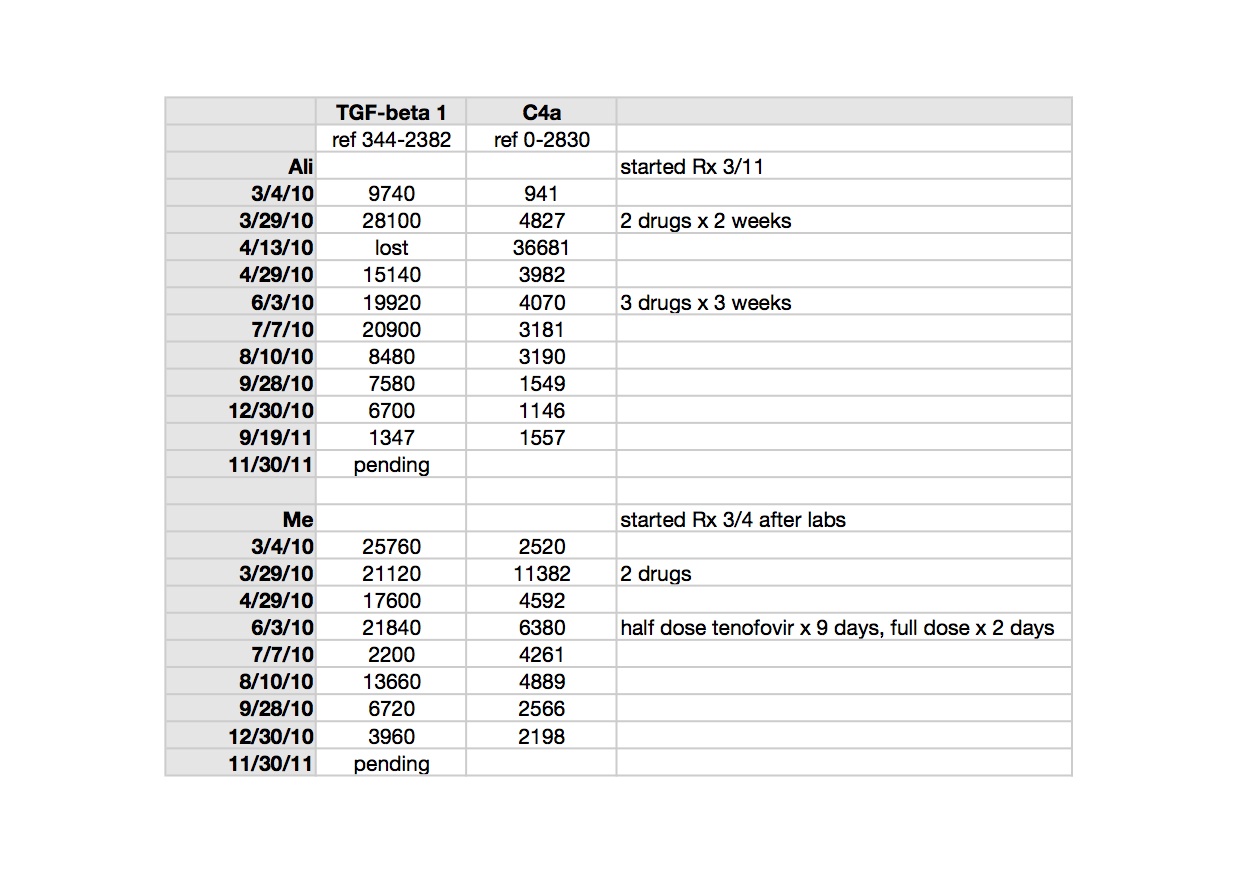
Many of the scientists came to read about Dr. Mikovits’ travails, but I am asking them to think about the science with us. In particular, I’d like to know your reactions to Dr. Snyderman’s data. Please adopt a handle and share with us. Your secret is safe with me. I ask you for the sake of the patients that you are now beginning to know, be bold. I realize that you are constrained by the knowledge that a patient community can do what we did, but there are 17 million patients worldwide in the ME/CFS cohort alone, who need creative thinking from you. There is every indication that our disease is reversible until it is very advanced. The unclaimed talent in the patient community is staggering, if only the disease could be calmed, not even cured. Look at me. I am productive after years of being almost unable to care for myself, let alone anyone else.
I would like to put an end to the discussion about the lab science in the Science paper, the WPI, VIP Dx. Nobody knows the answers, including the protagonists. I certainly have no basis for evaluating any of it. I defer to the scientific community to figure it out; discussing it here is not productive. At this point, it is non-contributory and boring. Take it someplace else. This is also not the place to argue about whether Dr. Mikovits should be canonized or not, though she is my friend, and I am very sorry for what is happening to her. But from a clinical point of view it is irrelevant. This blog is about developing a model for treatment and how to best live with the disease.
Thank you to our mold warriors for giving it another shot here, and for keeping it appropriate this time. I for one, think that your experiences of improvement without medication are significant. I also understand why you feel the need to tell others in the hope of reducing their suffering, as well as your frustration when you feel you aren’t being heard. I have been interested in Ritchie Shoemaker’s pioneering work, since 2002 when we shared a couple of patients with Ciguatera poisoning.
And a big thank you to In Vitro Infidelium for the considered comment this morning. No invective or politics at all. Just a reply about the scientific discussion at hand. It was a breath of fresh air. Thank you for the excellent paper by Voisset et al. The quote you lifted in your comment is precisely the point. Although it clearly isn’t a simple, straight forward infection, there is epidemiological evidence that it is an emerging disease of very great proportions, not a stable situation. AIDS isn’t simple and straightforward either, without a test, in that infected people can remain apparently healthy for a long time, or even indefinitely. Only a small percentage of people with HTLV ever become clinically ill from it. Inbred sick mice don’t get sick from their MLV’s, but wild mice and some other rodents can. All I am asking for is that it be studied, not shut down if this attempt fails. Also, that our therapeutic options not be limited by how slow the science will be to unfold, even in a best case scenario in which Dr. Lipkin finds something.
My hat is off to Dr. Lipkin. His finely worded communication to the patient community brought tears to my eyes. The only thing I would take exception with at all was the use of the word definitive. If by some quirk of fate, this study is completely negative, we beg you, use those specimens to take the next step.
Today’s song: Learning to Fly: by Tom Petty