I have to hand it to Dr.’s Switzer et al for responding to the vaccine question. Even if it was a very literal response, the findings were imparted clearly and believably. They looked for mouse viruses in 8 vaccines currently on the market. None of the vaccines were grown in mouse cells and, not surprisingly, they didn’t find any mouse viruses. No MLV’s at all in vaccines produced from chick, macaque, guinea pig or hamster cells. However, they did find human, avian and porcine endogenous retroviruses that they already knew were there, plus a new hamster virus in the vaccine grown in hamster cells… but it was DNA only, not a speck of RNA, so no worries… No Evidence of Murine Leukemia Virus-Related Viruses in Live Attenuated Human Vaccines. Switzer. Their conclusion: “We found no evidence of XMRV and MLV in eight live attenuated human vaccines further supporting the safety of these vaccines…”
Dr. Anon, PhD thinks I should do nothing for the next 10 years while I, my daughter and my patients deteriorate. We should all just wait while a bunch of jokers at the CDC try to figure out what the questions are. I know what the questions are. Anyone with critical thinking skills that has actually read what I have written on this blog (including the references) should know what the questions are. Whether or not one particular xenotropic MLV exists in humans or not is now quite besides the point. Not finding MLV’s in 8 vaccines that never came near a mouse cell doesn’t support the safety of anything. Even Switzer et al suggest that maybe they should look at batches of old vaccines, though my understanding is that they were mostly used up in the search for the origin of HIV. They also seem to think that maybe the monoclonal antibody folks should take a closer look into their products, e.g. rituximab, produced via an intentional fusion of mouse and human. They’ve been doing this since the ’70’s. Fooling Mother Nature. Would one of the scientists reading like to explain to us exactly how this is done? The literature is confusing.
But Dr. Anon, PhD, reading my blog, wants to “puke” because I am taking properly prescribed drugs for an off label indication? What a world! Tenofovir is prescribed for chronic Hepatitis B. Does that make you want to puke? We have non-HIV, non-HTLV AIDS, exactly analogous to non-A, non-B hepatitis before C was isolated. Wikipedia article: Off-label Use. The off-label prescribing of existing arv’s is completely legal. The only reason to prohibit it is because of the enormous financial implications if it works. Only a very few people have tried it. No disasters yet attributable to it, unlike most of the pharmaceutical alternatives; and to the scientists reading, you wouldn’t believe the dangerous crap my patients come to me taking, in combinations that have no research at all behind them to tell us about possible interactions. In my case, the only adverse effect of my experiment with arv’s that I can point to is that my straight hair became curly; this happens occasionally with chemotherapy and other drugs.
Tenofovir treats Hepatitis B. Raltegravir inhibits Herpesviruses. AZT has been noted to impact Sjogren’s, which seems to be overrepresented in our patient group. Protease inhibitors kill some parasites. I referenced a paper in the last blog in which it was reported that HAART brought about an impressive remission in a patient with advanced MS (and some of us, myself included, have MS light). Those “confounders” are good things about the drugs in clinical practice; all drugs have good things and bad things about them for a given individual. As a clinician, I love it when a drug hits two things in a patient, making it more likely that the cost/benefit ratio for that drug will be favorable for that person. However, the idea that my response to arv’s is because they controlled my Herpesviruses is almost as ludicrous as the idea that Dr. Snyderman’s cancer cells went down because of a placebo effect. Twice.
This seems like a good time to note that I have never had mono and am serologically negative for EBV. Since I was an ER doctor for 16 years and exposed to lots of mono, my body must be pretty good at keeping invaders out. Ali’s EBV tests are consistent with prior infection, and we both have low titer IgG for HHV-6, like almost everybody. There is really nothing to suggest that we have activated Herpesviruses as part of our picture, opportunistically or otherwise. Ali falls squarely into the Lyme group, not the activated virus group, and opportunistic infectious are not really a part of my clinical picture at all. I catch almost nothing. It’s the inflammatory effect of the physiological changes caused by the persistent immune shift to fight viruses so effectively that creates the subjective illness. Patients, and doctors, often confuse the symptoms of persistent inflammation with an active infection that needs to be killed or treated. There is also a subset of patients that catches everything and has ongoing problems with activated viruses. I have heard from people who have had mono and shingles numerous times.
Most novel uses of existing drugs are figured out serendipitously. Somebody with two things takes a drug for one thing and the other thing gets better. Occasionally, somebody actually connects some dots and tries something on purpose. If it gets reported, it is called a case study. In a sane world it would be followed with an open label trial and then a double blind placebo controlled study.
In response to the criticism that I’ve lead thousands of innocent patients down the garden path, please read what I’ve written, before jumping to conclusions. I have never said anyone should take arv’s. My point is that it should not be prohibited, and most definitely, the decision should not be in the hands of a bunch of lab scientists that have never treated a patient. A retrovirologist has no basis for an opinion about treatment at all. That they would presume to comment is a sign of disordered thinking right there.
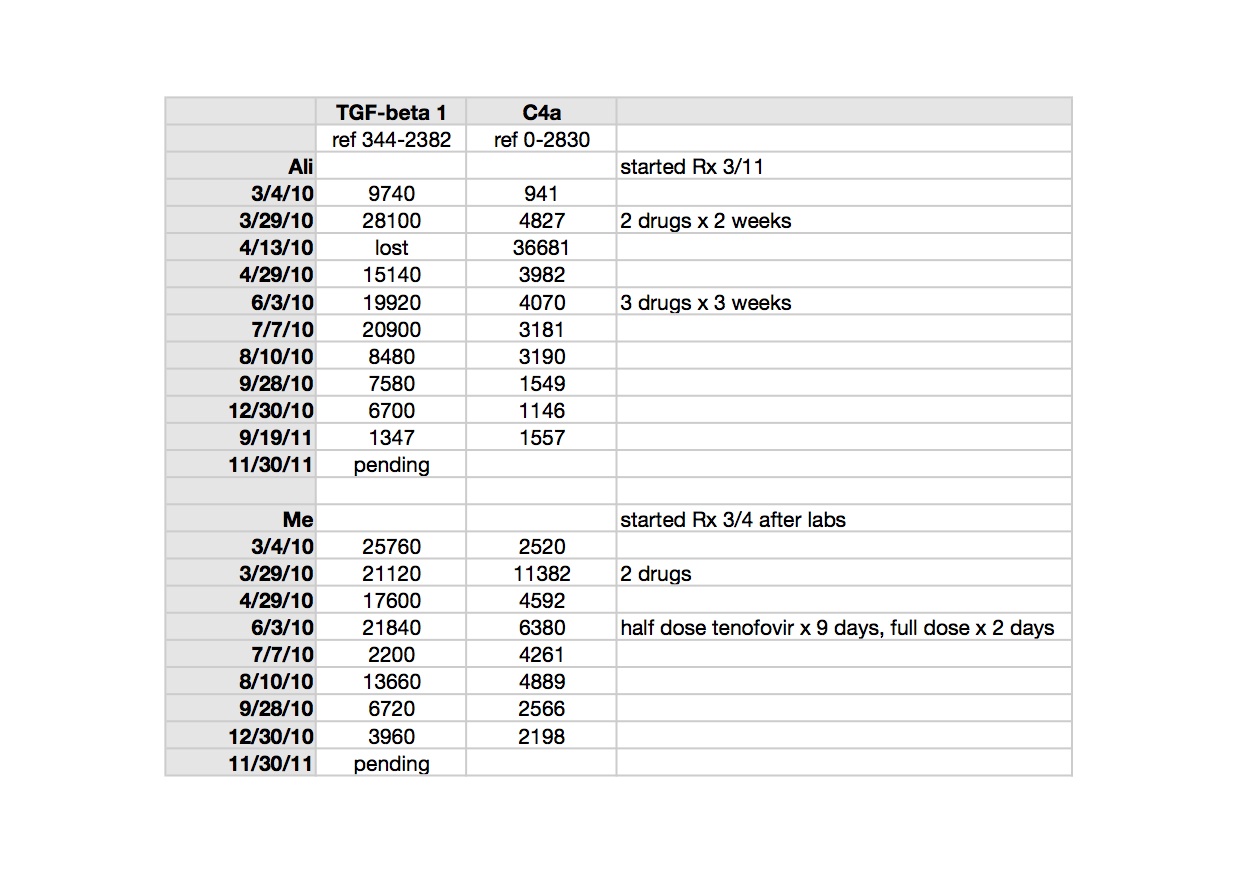
As I have said all along, ours was never a good experiment. What I have reported here is strictly clinical medicine. We were on an uphill course for about six months before starting arv’s, after quitting Lyme treatment. I do think that antibiotics were making us worse and when we stopped them, we went uphill, though an LLMD might say our treatment had worked:). I believe that arv’s helped us, though incompletely, not surprising for patients that have been sick for many years, who most likely have a high proviral load that continues to replicate mitotically. We still seem to be doing better than might be expected, but I have no way of knowing how we would be at this moment had we never taken them. The only marker we had to follow, TGF beta-1, initially very high has normalized for both of us over a year and a half (see numbers posted here; the pending results from 11/30 were normal TGF beta-1 and elevated C4a, for both of us). It is a very bad disease and we both feel lucky that our suffering is reduced. I wish that the science was keeping up so that we might have a better way of monitoring our therapy. We need a viral load measure or RT assay to follow, understanding full well that we might have more than one virus each and replication incompetent contributors. My biggest concern is the possibility of viral resistance, not toxicity of the drugs.
As far as the arv elist is concerned, I try to create a safe place for patients taking arv’s to discuss their experiences. Occasionally, I answer a question, but mostly, it is patients talking to patients. Everyone on the list, thirty or so of them, decided to take arv’s on their own, and all have their own prescribing doctors, except for a few that live outside of the US. In my practice, since I am willing to prescribe arv’s for an extremely informed patient, I must not be pushing it very hard, since none of my private patients have yet swallowed an arv.
Unfortunately, it is still the patients least likely to respond who are trying it, people who have been sick for a very long time with advanced disease that feel like they have nothing to lose. Much scarier to contemplate, but with a much greater possible upside, is the question of what would happen if newly crashed ME/CFS or ASD patients were treated quickly after onset of symptoms. This obviously needs to be investigated, but in a controlled setting. It will be very expensive to do safely, so is unlikely to happen for either of these conditions (cancer more likely). People don’t like to be wrong and there are lots of wrong, powerful people in this story.
My husband has been acting CFSy lately. When his symptoms flare, I am always impressed that it must be an infectious disease. All four members of my nuclear family have certain common symptoms, e.g. painless ocular migraine, which was a rare condition when I was an ER doctor 17 years ago, and orthostatic intolerance, of a form that nobody had ever heard of a few decades ago. Vascular instability and autonomic neuropathy in four members of a nuclear family, two sick, two not. Husband and wife not even distantly related. I thank God every day that my son isn’t autistic. I vaccinated him selectively, for the wrong reasons, but I have heard from that woman out there who, like me, has CFS and a CFS daughter, plus an autistic son. Is it because I didn’t give him the Hep B vaccine (which is not a live vaccine, but causes persistent immune activation over a long period of time)?
I get letters now and then suggesting that I do not know how horrible polio and other infectious diseases were before vaccines. That isn’t true, I do know. But just because the vaccine program saved many people doesn’t mean that we shouldn’t look at problems that may have been caused by it, and modify our recommendations now for people at high risk, e.g. people with CFS and new offspring of ME/CFS women. We desperately need extensive epidemiological studies to find out what happened when. If you want to look at the bigger evolutionary picture, we have changed nature’s culling process. If you take the starfish parable from a few blogs back to it’s natural conclusion, throwing the starfish back is a mistake, because they are vicious predators that overbreed and damage the reef.
In the meantime, the backlash from the flash of illumination has started. The Mayo Clinic says SSRI’s (which many ME/CFS patients don’t tolerate), sleep meds, GET and ‘therapy’ are what we can have as far as treatment goes. That’s the best they can do for a million sick people? On their website: “More than 3,300 physicians, scientists and researchers from Mayo Clinic share their expertise to empower you to manage your health.” Shame on them. May the doctors that came up with this page never have to get sick, or have their child get sick, with a horrible debilitating disease and be faced with such options. May they find some shred of compassion in their hearts of stone before that fate can befall them.
I am writing to you today from the Louisiana bayou. My husband’s 50th birthday present a couple of months ago was our first RV, and this is our first trip. We have always wanted to try the RV lifestyle, but now even more so, since we love to be in nature and it is the only way that I can still travel comfortably. Our son was just accepted to Tulane with a big scholarship, so we decided to take him to New Orleans to help him decide what he wants to do. Ali didn’t come on this trip, but will come on the next one, shorter and closer to home. The trip has been exciting, to say the least. We survived the worst blizzard in 40 years in north Texas and a tornado warning in southern Louisiana.
I love the spontaneity and limitless possibility of seeing the world this way. Change is usually so difficult with this illness, but everything I need is close at hand and comes with us when we move. The pendulum of my disease continues to swing, as always, while I practice the art of transcending symptoms, living as many full moments as I can. Right now, my husband and son are fishing in the rain. We’ve had the worst luck with weather. Adversity is giving us all the opportunity to practice acceptance and work on our interactions in a close space. Like life, the difficulties have been punctuated by amazing moments; yesterday we watched from our canoe as a small otter caught and fought a huge fish, then defended it from a Great Blue Heron. This part of the country is very wild and alive. When I couldn’t sleep for a while last night, I listened to wonderful, unfamiliar night noises.
And the breaking news? Lo et al just retracted, saying the work was perfect, but the conclusion must be wrong, since nobody has replicated it yet, except for one other lab. Therefore, enough money wasted. Now there’s some ironclad logic for you.
Tonight’s song: The Wild Goose
by Kate Rusby