From Shakespeare’s King Henry V, Act III, Scene I
King Henry V:
Once more unto the breach, dear friends, once more;
Or close the wall up with our English dead.
In peace there’s nothing so becomes a man
As modest stillness and humility:
But when the blast of war blows in our ears,
Then imitate the action of the tiger;
Responding to the flurry of concern for my feelings and irritation from readers about negative comments left by angry Anonymous people, personally, I welcome the discussion, even if expressed without courtesy. There is much to be learned by considering the things the opposition is thinking. Their need for anonymity is amusing and speaks for itself. Don’t let them get you down. Keep your friends close and your enemies closer. It’s all grist for the mill.
As far as I know, the WPI, which is a non-profit, has no conflict of interest. The mission is clear and the people dedicated to the cause. The individuals at the WPI have waived their IP (intellectual property) rights in favor of the institute. Should VIP Dx ever make a profit, it all goes to the institute also. I challenge the other characters in this story to say the same.
As for everyone using their inside voices until the science runs it’s proper course, that’s just naive. That’s like saying that our newspaper reporters are only reporting the truth. People are people. They ask the questions they want answered, and they frame those questions in such a way that the answers will spin it the way they like. That’s why blinding is necessary for the scientific method.
I received an email this morning from Michael Snyderman that I am copying here with his permission:
There is a conflict interest here. A major player is a very wealthy woman by the name of Kristin Loomis who with Annette Whittemore founded the HHV-6 Foundation. Loomis is a great believer that Herpes 6 causes CFS and a lot of other disease. Both women had children with CFS.
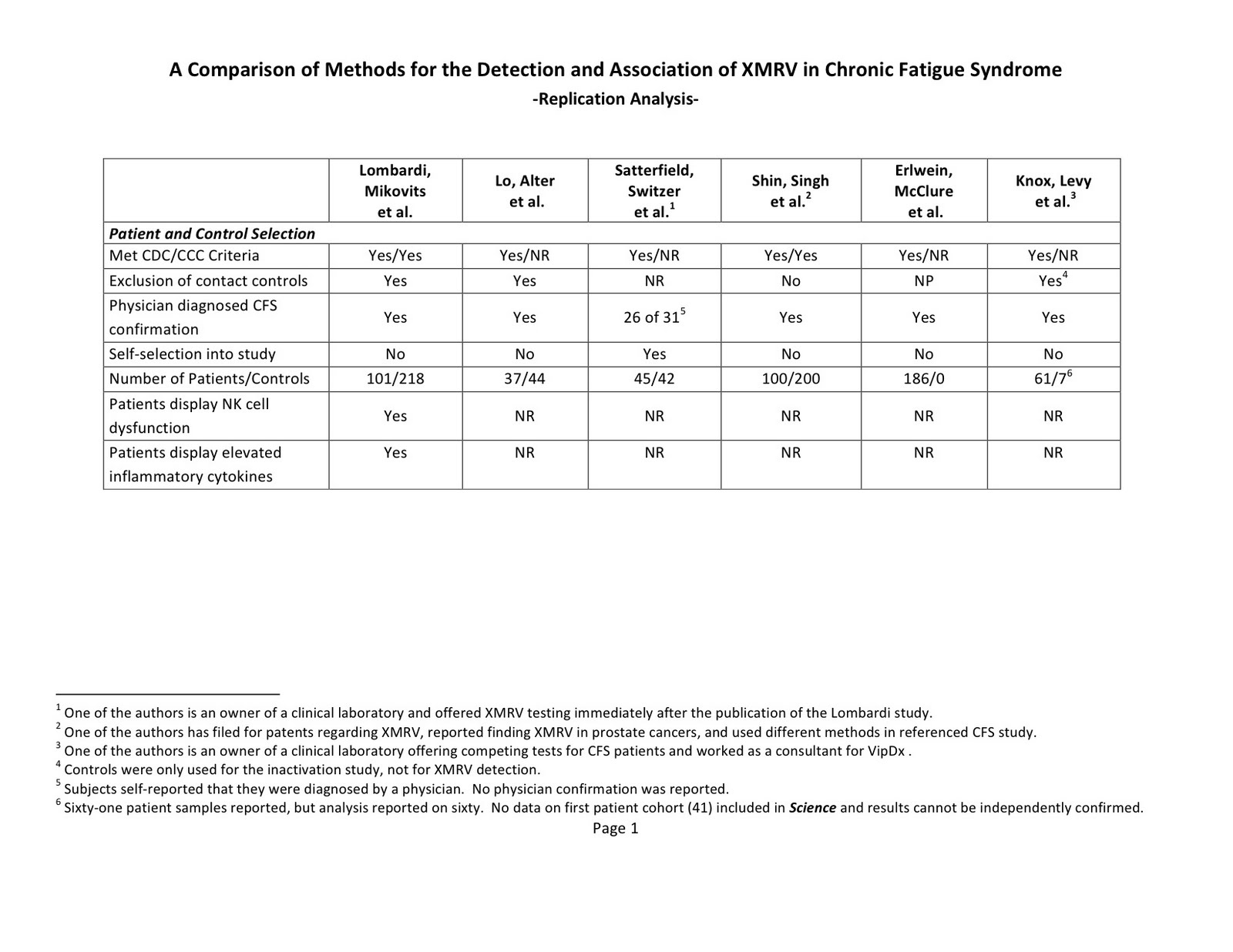
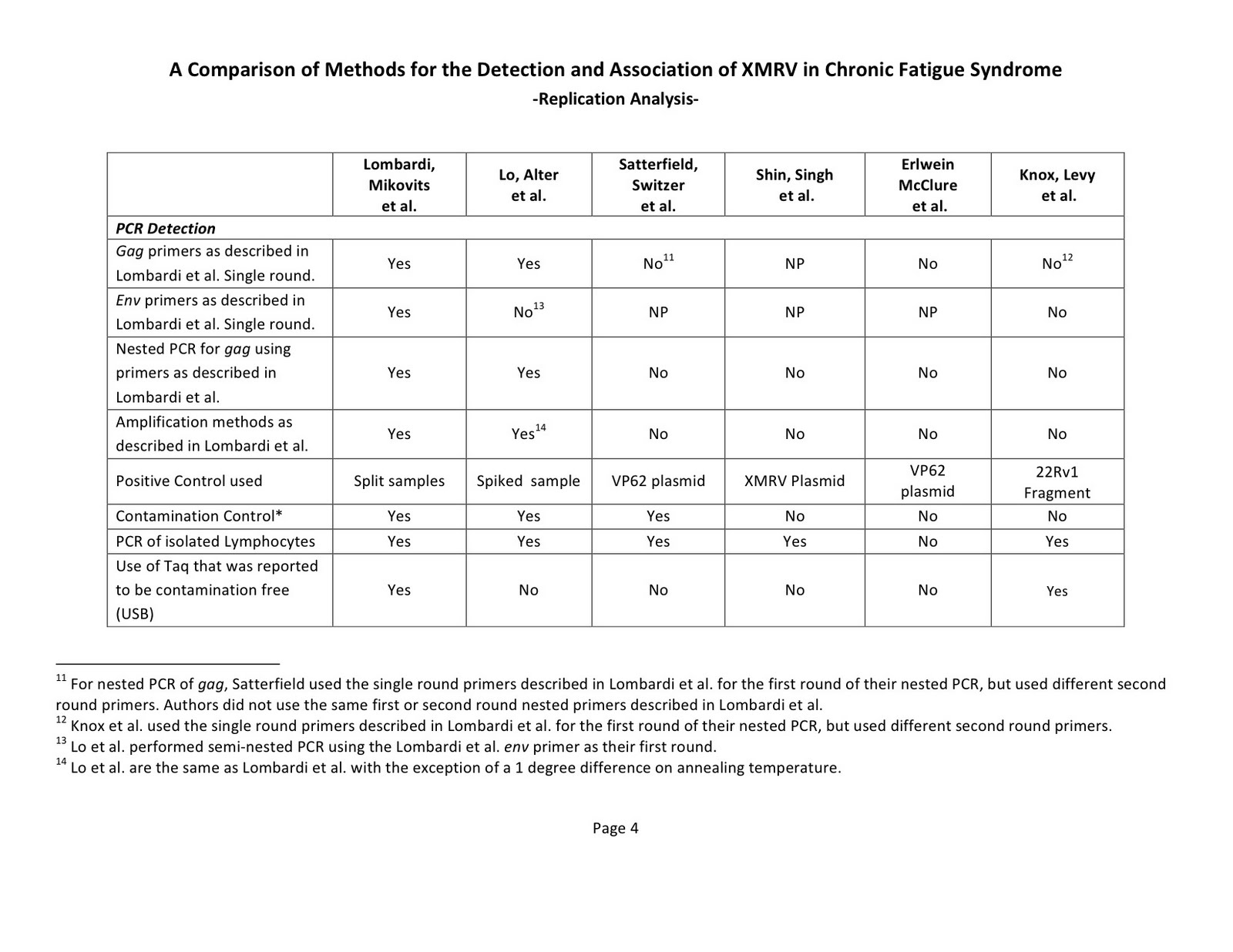
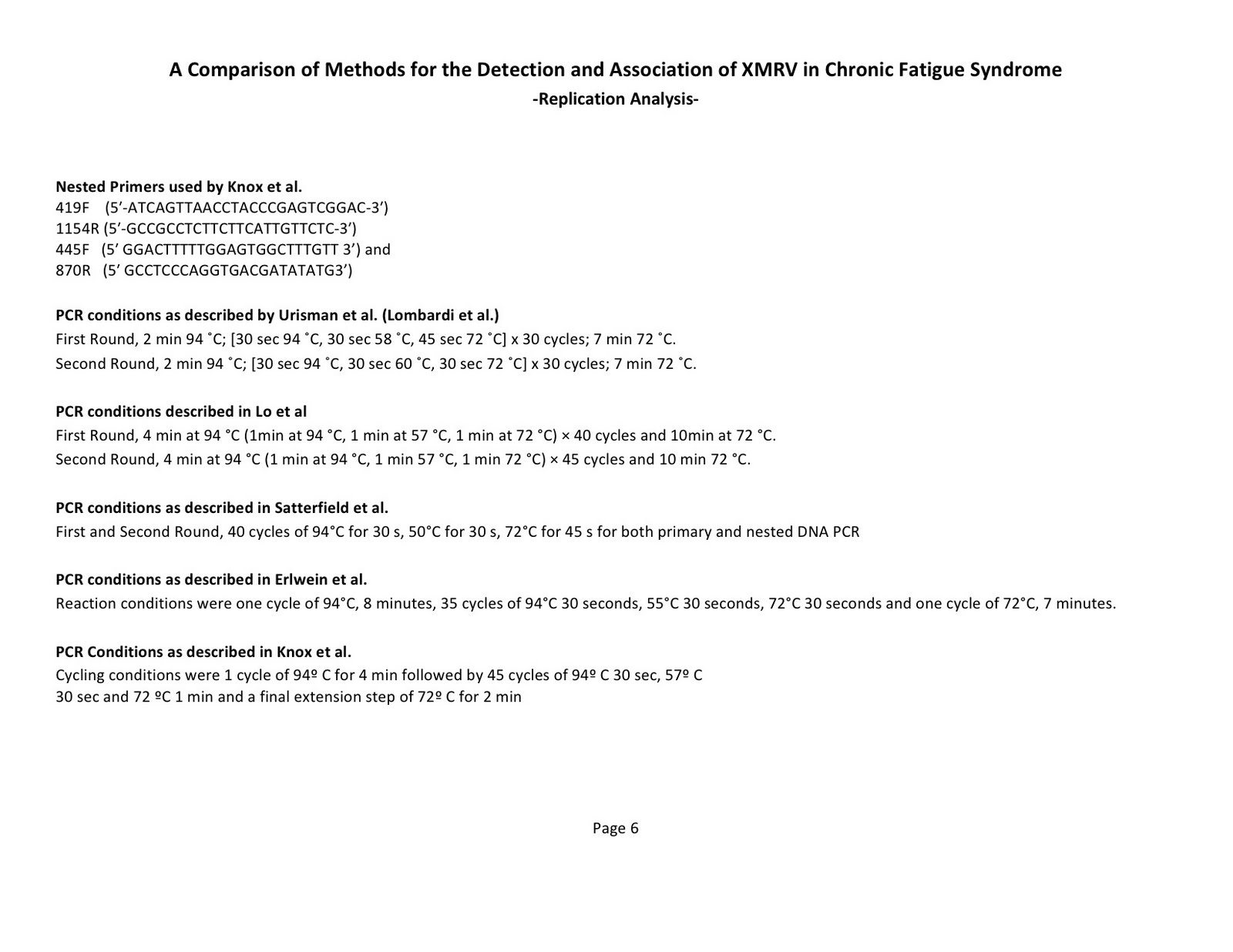
Whittemore later set up the WPI with Daniel Peterson who gave the WPI its original CFS samples. Initially the WPI was going to further the cause of Herpes 6. They had a scientist, Konnie Knox and Peterson who were from the HHV-6 Foundation and continued to get money from the HHV-6 Foundation. Knox was fired from the WPI. About this time Lombardi et al. found XMRV (arguably a poor name). Peterson was disturbed because he was a believer in Herpes 6. He left soon after the Lombardi et al. report came out. The position of the HHV-6 Foundation is that Herpes 6 is the cause of CFS and not XMRV and indeed that XMRV does not exist. Peterson then gave Knox the samples from his patients that she reported as negative in the new Science article. She did not declare any conflict of interest over her funds from the HHV-6 Foundation or the fact that she had been fired from the WPI.
There is more. The other article in Science is by John Coffin from Tufts. He first reported that XMRV was a contaminant in 2010. His colleague at Tufts is Brigitte Huber and she was a coauthor on this paper.
On the Tufts website Huber is listed as getting a grant from the HHV-6 Foundation:
Huber, Brigitte HHV-6, EBV and Endogenous Retrovirus in Patients with CFS HHV-
6 Foundation 11/1/09 – 4/30/10This grant was received right after the Lombardi et al. Science report in 2009. Coffin also did not declare any conflict of interest in his Science article although he had collaborated closely with Huber and was a colleague with her at Tufts.
The bottom line is that drug companies will not develop drugs that will help us if they believe that XMRV and related MLRVs do not exist. Lives could be saved with just one type of drug, a protease inhibitor – the one for HIV doesn’t work for XMRV and is a key category of drug for treatment of MLRV-related disorders as proteins such as env are not countered by raltegravir and the RT inhibitors.
Michael Snyderman, MD
Also from my morning mail:
My dr. and I have mostly contact by email because I am bedbound and cannot get to the office as much as I should. This morning I received an email from him … he made the remark that it is very interesting to him that WPI was asked to retreat their paper. Than he proceeded to tell me that he ran some test in his office and that WPI was mistaken to tell me I am XMRV positive because his test came out negative from the other…
How can that be? I feel like the ground has been pulled from under me. The hope I had to finding a solution for my 30 years of suffering is gone! How is it possible that a regular physician who specializes in ME/CFS and Fibromyalgia can do a test like this? I’m gobsmacked and feel myself tunneling in a deep depression. Everything I believed in he took away from me with just one sentence, I just can not stop crying and am so upset.
WPI tested me positive and I have been holding on to that, because I didn’t have much hope elsewhere. I don’t know what to do now. There isn’t any hope left for me.
One of the many sad things happening is that the only testing available may not yet be sensitive enough. Or it may be sensitive enough, but some of us have different viruses that cause clinically indistinguishable disease from the XMRV positive patients. The current VIP Dx serology is aimed at xenotropic and polytropic MLV’s and is not positive in everyone one would expect if the test picks up every infected patient or if XMRV was the only cause of CFS. VIP Dx has a test. It comes out positive or negative. But like many tests, it’s not that black and white. Like all lab tests, it must be interpreted by a doctor within the context of a complete clinical picture, and an understanding of the state of the testing with respect to a particular disease. At this point in time, it’s that test or nothing. Nothing is a valid choice. It is a personal matter. But why the invective? Nobody has to use VIP Dx that doesn’t want to.
As I’ve said before. I could be wrong about anything. Like everyone, I interpret what comes my way from my own perspective. I am not a retrovirologist or even a scientist. I’m a doctor who is fluent with the literature. I also have the disease and my daughter has the disease. Why does my sharing my opinions and experiences make some people so angry, when the vast majority seem to benefit from hearing my thoughts? I challenge any of the people I’ve criticized to come forward as themselves and tell us what happened from your perspective. My mind can change. I’d love to think that everyone involved has integrity and is motivated by the right things, but human beings being what they are, that isn’t likely. As I keep saying, I am wedded to nothing but the truth. And time is of the essence.
This abstract by Prosperi et al may be of importance and I look forward to the paper. It seems confirmation in concept of what I suspect, that 22Rv1 isn’t the one in a trillion recombination event described in Paprotka et al. Interestingly the et al includes William Switzer who published a 0/0 study with Satterfield, as discussed in a previous blog here.
Murine leukemia viruses (MuLV) and Xenotropic MuLV-related viruses exhibit inter-tropic complex recombination patterns. Prosperi/Salemi
Given the evidence of inter-tropic recombination in MuLV, detection and classification of recombination in XMRV using different MuLV tropism prototypes should be interpreted with caution. Despite using a small dataset, a strong phylogenetic signal in the alignments and highly resolved phylogenies inferred both by full-length and sliding-window approaches, different recombination programs reported conflicting results. These results suggest that identification of parental strains of the potential recombinants is difficult and that recombination in the highly genetically related MuLV have been occurring for some time.
The hysteria in the media about the thousands of patients taking AIDS drugs is a joke. If that had happened, we’d have learned a lot, but they shut it down pretty effectively. I still don’t understand the inordinate fear of these particular drugs. All drugs have side effects. Every prescription has a potential cost/benefit ratio that has to be considered by the doctor and the patient at a particular moment. All options should be considered for a disease with no cure that produces such tremendous suffering. This was a prohibition from the beginning, such that taking antiretrovirals feels almost like a form of civil disobedience. As I said at the beginning, what if it works? Why does the scientific community not want to know, irrespective of the detection problems and their horror at skipping beyond their deductive reasoning process, clutched to their breasts like a religious totem? I know of about 50 patients taking arv’s, one to three drugs, for varying lengths of time. All have been sick for a long time. About a third feel they are improved. The rate of change is slow. I don’t know of anyone who has been seriously harmed, other than self-limited adverse reactions in the very early part of treatment. Some people who haven’t done well have gone off. As far as I know, everyone is getting proper monitoring. The interference in the physician patient relationship, happening on a grand scale with respect to restricting this particular treatment, is a travesty.
I have gone from sofa bound to very high functioning in 15 months, while taking antiretrovirals. It was not a good experiment however, nor have I ever claimed otherwise. I am more of an atypical MS picture than classic ME/CFS (like Ali), and I was already on an upswing since quitting lots of Lyme and symptom based treatment six months prior, but still very sick and essentially non-functional. I have also started other medication since, Deplin and Actos. I feel safe in saying that arv’s haven’t hurt me, including a year of AZT. In no way am I suggesting that anyone should do what I did, but everyone should have the right to consider it. The scariest potential risk is renal failure from tenofovir, a very rare event in the HIV world, seen primarily in people with preexisting renal problems. There are some long term consequences of AZT that need consideration. Proper monitoring is necessary.
I’ve returned to practice on the Big Island in Hawaii, because that’s where my active license is, and because I love it there. I trained in Honolulu, after medical school in the Bronx, and had my first job there. I’ve been licensed since 1980, always hoping to return. My family has recently grown to include my eldest daughter (who is adopted and very healthy) and my two small grandchildren. My son has a year of high school to go in Santa Fe. Moving everybody right now is out of the question. And I’m still traveling to Reno also. My husband and I are adapting to the fact that we will be spending a lot of time apart, after 23 years of marriage without separation. I am profoundly grateful to be able to contribute again. When I was practicing in Great Barrington, I was at 90% and it was all about the 10%. Now 90% feels like 110%. When pain goes away, it’s better than if you’d never experienced pain in your life. So round 3 for me. The comeback kid. Who better to treat it? I know the enemy intimately.
I wish it were Ali and not me that was better enough to reenter. I have tremendous survivor’s guilt writing this. My impression is that the second generation is sicker. Simple retroviruses can endogenize or maybe it’s just worst to get it before your immune system is developed. I have heard of very small children who sound like they have full-blown CFS (Beethoven’s 9th symphony?), 4 being the youngest. Not autistic. ME/CFS. 3rd generation.